University of Oslo, Oslo, Norway.
Department of Vascular Surgery, Akershus University Hospital, Lørenskog, Norway.
Cardiovasc Diabetol. 2024 Sep 9;23(1):333. doi: 10.1186/s12933-024-02421-w.
The aim was to investigate the total prevalence of known and undiagnosed diabetes mellitus (DM), and the association of DM with perioperative complications following elective, infrarenal, open surgical (OSR) or endovascular (EVAR), Abdominal Aortic Aneurysm (AAA) repair.
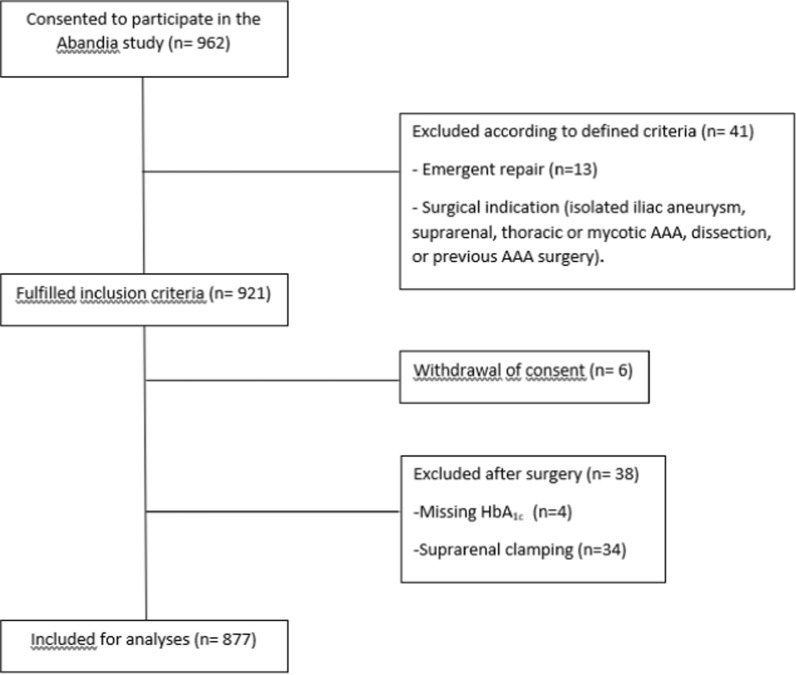
In this Norwegian prospective multicentre study, 877 patients underwent preoperative screening for DM by HbA measurements from November 2017 to December 2020. Diabetes was defined as screening detected HbA ≥ 48 mmol/mol (6.5%) or previously diagnosed diabetes. The association of DM with in-hospital complications, length of stay, and 30-day mortality rate were evaluated using adjusted and unadjusted logistic regression models.
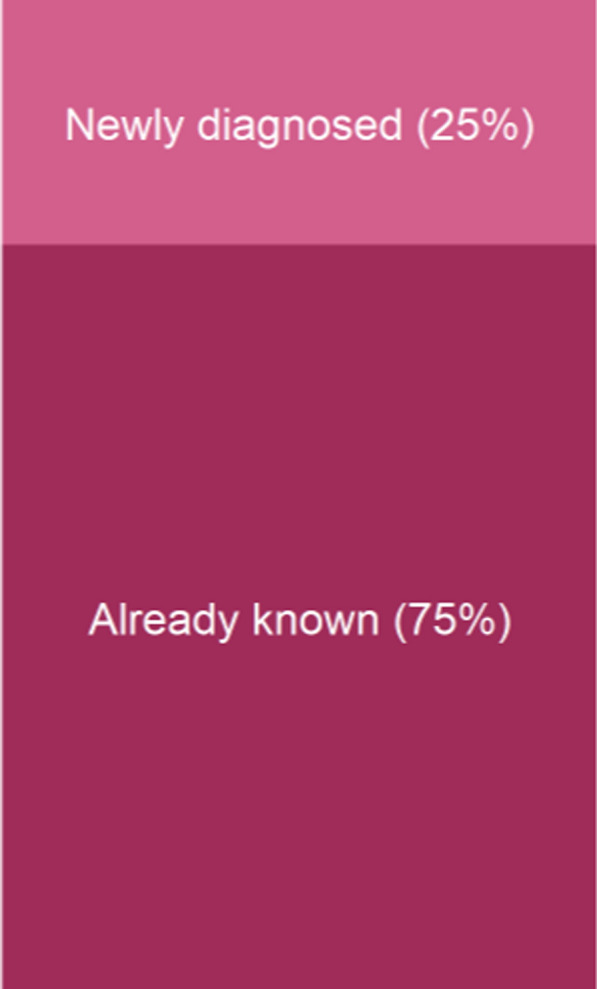
The total prevalence of DM was 15% (95% CI 13%,17%), of which 25% of the DM cases (95% CI 18%,33%) were undiagnosed upon admission for AAA surgery. The OSR to EVAR ratio was 52% versus 48%, with similar distribution among DM patients, and no differences in the prevalence of known and undiagnosed DM in the EVAR versus the OSR group. Total 30-day mortality rate was 0.6% (5/877). Sixty-six organ-related complications occurred in 58 (7%) of the patients. DM was not statistically significantly associated with a higher risk of in-hospital organ-related complications (OR 1.23, 95% CI 0.57,2.39, p = 0.57), procedure-related complications (OR 1.48, 95% CI 0.79,2.63, p = 0.20), 30-day mortality (p = 0.09) or length of stay (HR 1.06, 95% CI 0.88,1.28, p = 0.54). According to post-hoc-analyses, organ-related complications were more frequent in patients with newly diagnosed DM (n = 32) than in non-DM patients (OR 4.92; 95% CI 1.53,14.3, p = 0.005).
Twenty-five percent of all DM cases were undiagnosed at the time of AAA surgery. Based on post-hoc analyses, undiagnosed DM seems to be associated with an increased risk of organ related complications following AAA surgery. This study suggests universal DM screening in AAA patients to reduce the number of DM patients being undiagnosed and to improve proactive diabetes care in this population. The results from post-hoc analyses should be confirmed in future studies.
本研究旨在调查择期、肾下、开放手术(OSR)或血管内(EVAR)腹主动脉瘤(AAA)修复术后已知和未确诊的糖尿病(DM)的总患病率,以及 DM 与围手术期并发症之间的关系。
在这项挪威前瞻性多中心研究中,877 名患者于 2017 年 11 月至 2020 年 12 月期间通过 HbA 测量进行术前 DM 筛查。DM 的定义为筛查发现 HbA≥48mmol/mol(6.5%)或既往诊断为糖尿病。使用调整和未调整的逻辑回归模型评估 DM 与住院期间并发症、住院时间和 30 天死亡率之间的关系。
DM 的总患病率为 15%(95%CI 13%,17%),其中 25%的 DM 病例(95%CI 18%,33%)在 AAA 手术入院时未被诊断。OSR 与 EVAR 的比例为 52%比 48%,DM 患者之间的分布相似,EVAR 组和 OSR 组中已知和未确诊 DM 的患病率无差异。总 30 天死亡率为 0.6%(5/877)。58 名(7%)患者发生 66 例与器官相关的并发症。DM 与住院期间与器官相关的并发症(OR 1.23,95%CI 0.57,2.39,p=0.57)、手术相关并发症(OR 1.48,95%CI 0.79,2.63,p=0.20)、30 天死亡率(p=0.09)或住院时间(HR 1.06,95%CI 0.88,1.28,p=0.54)之间无统计学显著相关性。根据事后分析,与非 DM 患者相比,新诊断的 DM 患者(n=32)的器官相关并发症更为频繁(OR 4.92;95%CI 1.53,14.3,p=0.005)。
在 AAA 手术时,25%的 DM 病例未被诊断。根据事后分析,未确诊的 DM 似乎与 AAA 手术后与器官相关的并发症风险增加有关。本研究建议对 AAA 患者进行普遍的 DM 筛查,以减少未确诊的 DM 患者数量,并改善该人群的主动糖尿病管理。应在未来的研究中证实事后分析的结果。