Khan Naveed N, Zurayyir Elaf J, Alghamdi Afyaa M, Alghamdi Sara F, Alqahtani Mohammed A, Abdalla Esra M, Jurays Najwa S, Alassiri Abdullah M, Alzahrani Hatoon A, Althabet Abdullah A
Internal Medicine, King Salman Armed Forces Hospital, Tabuk, SAU.
College of Medicine, Jazan University, Jazan, SAU.
Cureus. 2024 Aug 12;16(8):e66694. doi: 10.7759/cureus.66694. eCollection 2024 Aug.
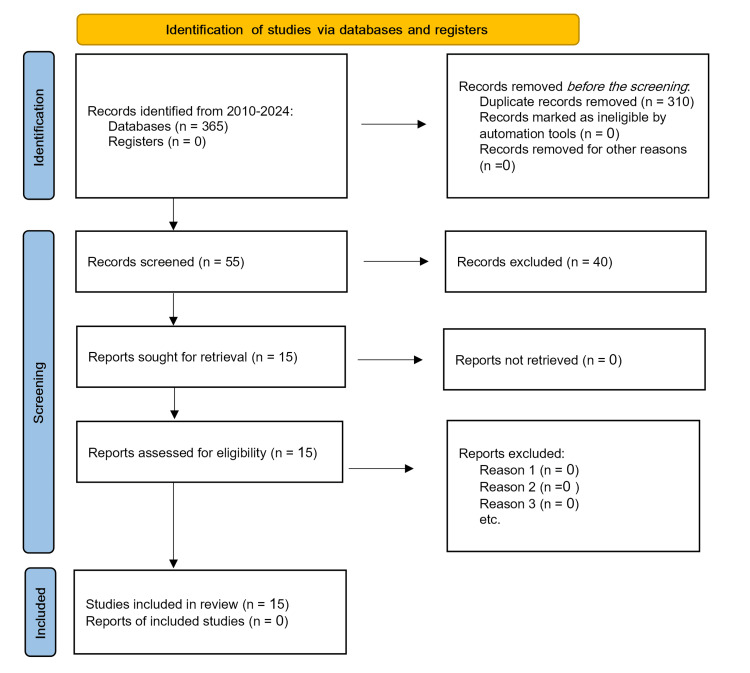
A hypertensive crisis is defined as a sudden and significant rise in blood pressure. The blood pressure reading is 180/120 mmHg or higher. A hypertensive crisis is a medical emergency. It can lead to a heart attack, stroke, or other life-threatening medical problems. Investigating the management of the hypertensive crisis was the goal of this study. English-language articles were collected from 2010 to 2024 demonstrating the management of the hypertensive crisis. Overall, there were 15 articles. Surveys and analyses of national databases were the most widely used methods (n=15). The scientific studies documented (1) all investigative studies or reports that included a hypertensive crisis diagnosis, (2) data integrity and reproducibility, and (3) management studies. Other studies show that acute severe hypertension in the hospital is associated with high rates of mortality and morbidity, particularly with new or worsening end-organ damage. The problem is linked to poor medical adherence, but alarmingly low follow-up rates are likely to contribute to a high recurrence rate. The treatment of acute severe hypertension varies according to the hospital unit (medical ward or intensive care unit), medication, and blood pressure targets or thresholds. Because of a lack of evidence-based guidance, arbitrary blood pressure control targets are used, or blood pressure targets are crudely extrapolated from guidelines intended primarily for outpatient management. Patients with acute aortic dissection need to be administered intravenous esmolol within 5 to 10 minutes in order to lower their blood pressure right away. The goal is to maintain a systolic reading of less than 120 mm Hg. Vasodilators such as nitroglycerin or nitroprusside may be administered if the blood pressure persists following beta blocking. Intravenous administration of clevidipine, nicardipine, or phentolamine is required; the initial dose is 5 mg, with subsequent doses given every 10 minutes as necessary to achieve the desired reduction in blood pressure.
高血压危象定义为血压突然大幅升高。血压读数为180/120 mmHg或更高。高血压危象是一种医疗急症。它可导致心脏病发作、中风或其他危及生命的医疗问题。本研究的目的是调查高血压危象的管理。收集了2010年至2024年期间关于高血压危象管理的英文文章。总共15篇文章。对国家数据库的调查和分析是使用最广泛的方法(n = 15)。这些科学研究记录了:(1)所有包含高血压危象诊断的调查研究或报告;(2)数据完整性和可重复性;(3)管理研究。其他研究表明,医院内的急性重度高血压与高死亡率和发病率相关,尤其是与新出现的或恶化的靶器官损害有关。这个问题与医疗依从性差有关,但令人担忧的是,极低的随访率可能导致高复发率。急性重度高血压的治疗因医院科室(内科病房或重症监护病房)、药物以及血压目标或阈值而异。由于缺乏循证指南,使用的是任意的血压控制目标,或者血压目标是从主要针对门诊管理的指南中粗略推断出来的。急性主动脉夹层患者需要在5至10分钟内静脉注射艾司洛尔,以便立即降低血压。目标是将收缩压维持在120 mmHg以下。如果在使用β受体阻滞剂后血压仍持续升高,可给予硝酸甘油或硝普钠等血管扩张剂。需要静脉注射氯维地平、尼卡地平或酚妥拉明;初始剂量为5 mg,必要时每10分钟给予后续剂量以达到预期的血压降低效果。