Razavian Niema B, Waltonen Joshua D, Steber Cole R, Shenker Rachel F, May Nelson H, Yang Jae H, Lanier Claire M, Greven Kathryn M, Frizzell Bart A, Hughes Ryan T
Department of Radiation Oncology, Wake Forest School of Medicine, Winston-Salem, North Carolina, USA,
Department of Radiation Oncology, H. Lee Moffitt Cancer Center, Tampa, Florida, USA,
ORL J Otorhinolaryngol Relat Spec. 2024;86(3-4):140-150. doi: 10.1159/000541390. Epub 2024 Sep 12.
Strategies for treatment of tonsil carcinoma are under active investigation. Limiting surgical and radiation treatment volumes to the primary tumor and ipsilateral neck in appropriately selected patients are one such approach. Here, we present our institutional experience with treatment through ipsilateral surgical or radiotherapeutic neck management.
We retrospectively reviewed our institutional database of patients with tonsil carcinoma treated from 2012 to 2020. Patients were included for analysis if they received definitive radiation therapy (RT), definitive surgery (S), or surgery with postoperative radiation therapy (S-PORT) and whose treatment volumes were limited to the primary tumor and involved/elective ipsilateral neck. Patients who received radiation and/or surgery to the contralateral neck (including those with bilateral nodal involvement), as well as patients with metastatic disease, were excluded. Clinical factors including T- and N-stage (AJCC 7th edition), and HPV status (by p16 and/or HPV DNA PCR) were recorded, as were pathologic factors (when applicable) including margin status, extracapsular extension (ECE), lymphovascular invasion (LVSI), and perineural invasion (PNI). Overall survival (OS), progression-free survival (PFS), and locoregional control (LRC) at 2 years were estimated using the Kaplan-Meier method.
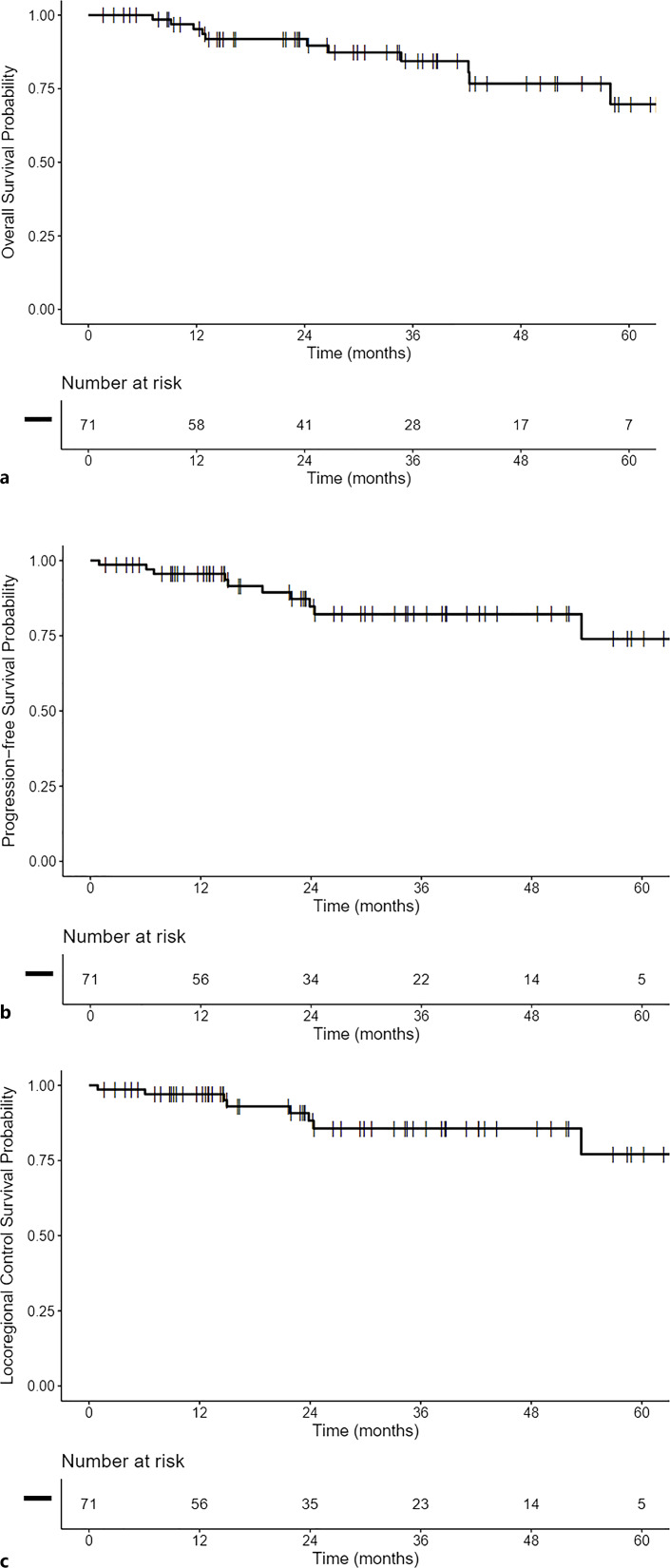
In total, 71 patients were treated with unilateral neck approaches: S (n = 49), RT (n = 10), and S+PORT (n = 12). Among these patients, 32, 36, and 3 had T1, T2, and T3 disease, respectively. N-stage was N0, N1, N2a, N2b, and N3 in 22, 20, 5, 23, and 1 patient(s), respectively. Concurrent chemotherapy was administered in 12 patients. From those with recorded risk factors, 86% were HPV positive, 20% had LVSI, 7% had PNI, 13% had ECE, and 5% had positive margins. From a median follow-up of 27 months, local, regional, and distant failures occurred in 5, 6, and 5 patients, respectively. No contralateral neck failures were recorded. At 2 years, OS, PFS, and LRC were 92% (95% CI 85-99%), 85% (95% CI 75-95%), and 88% (95% CI 80-98%), respectively.
In patients with early T-stage tonsil carcinoma, treatment of the primary tumor and ipsilateral neck is associated with acceptable OS, PFS, and LRC. In this population, the risk of contralateral neck failure is likely very low regardless of primary treatment modality. Additional prospective studies are needed to determine the impact of limiting treatment extent, either surgical or radiotherapeutic, to the unilateral neck.
扁桃体癌的治疗策略正在积极研究中。在适当选择的患者中将手术和放疗范围限制在原发肿瘤和同侧颈部是其中一种方法。在此,我们介绍我们机构采用同侧手术或放射治疗颈部管理的治疗经验。
我们回顾性分析了2012年至2020年在我们机构接受治疗的扁桃体癌患者数据库。如果患者接受了根治性放疗(RT)、根治性手术(S)或术后放疗的手术(S-PORT),且其治疗范围仅限于原发肿瘤和受累/选择性同侧颈部,则纳入分析。接受对侧颈部放疗和/或手术的患者(包括双侧淋巴结受累的患者)以及有转移性疾病的患者被排除。记录临床因素,包括T分期和N分期(美国癌症联合委员会第7版)以及HPV状态(通过p16和/或HPV DNA聚合酶链反应),以及病理因素(如适用),包括切缘状态、包膜外扩展(ECE)、淋巴管浸润(LVSI)和神经周围浸润(PNI)。使用Kaplan-Meier方法估计2年时的总生存期(OS)、无进展生存期(PFS)和局部区域控制率(LRC)。
共有71例患者采用单侧颈部治疗方法:手术(n = 49)、放疗(n = 10)和手术加术后放疗(n = 12)。在这些患者中,分别有32例、36例和3例为T1、T2和T3期疾病。N分期分别为N0、N1、N2a、N2b和N3的患者有22例、20例、5例、23例和1例。12例患者接受了同步化疗。在有记录的危险因素的患者中,86%为HPV阳性,20%有LVSI,7%有PNI,13%有ECE,5%切缘阳性。中位随访27个月时,分别有5例、6例和5例患者发生局部、区域和远处复发。未记录到对侧颈部复发。2年时,OS、PFS和LRC分别为92%(95%CI 85-99%)、85%(95%CI 75-95%)和88%(95%CI 80-98%)。
在早期T分期的扁桃体癌患者中,原发肿瘤和同侧颈部的治疗与可接受的OS、PFS和LRC相关。在该人群中,无论初始治疗方式如何,对侧颈部复发的风险可能非常低。需要更多的前瞻性研究来确定将手术或放疗的治疗范围限制在单侧颈部的影响。