Liu Qi, Wu Liusheng, Wang Xiangyu, Feng Yu, Wang Ying, Yan Jun, Li Xiaoqiang
Department of Thoracic Surgery, Peking University Shenzhen Hospital, Shenzhen, 518036, China.
Department of Graduate School, Zunyi Medical University, Zunyi, 563000, China.
Discov Oncol. 2024 Sep 13;15(1):442. doi: 10.1007/s12672-024-01307-3.
Controversy surrounds the treatment of visceral pleural invasion in lung cancer, and no studies have compared the efficacy of its four main treatment options (i.e., surgery, chemotherapy, targeted therapy, and immunotherapy). This study aims to compare and analyze surgery, chemotherapy, targeted therapy, and immunotherapy outcomes and explore the optimal treatment of visceral pleural invasion in lung cancer.
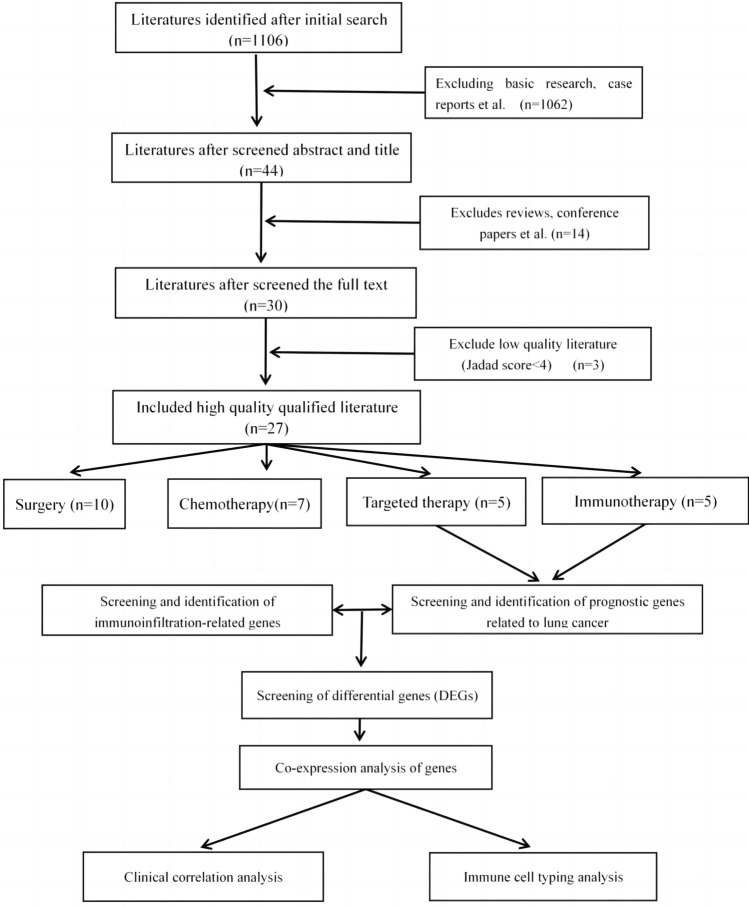
We searched electronic databases (i.e., Pubmed, Embase, Cochrane Library, CNKI, and Chinese Biomedical Literature Database Search) for relevant studies of treatment options for patients with visceral pleural invasion in stage IIA-IIB lung cancer. Searches times were limited to studies published between January 1, 2000 and February 20, 2021. Meta analysis was performed using RevMan 5.3 software We also downloaded original RNA transcription data about lung cancer invasion in the GEO and TCGA tumor databases, and used R 4.0.3 software to perform differential expression and co-expression gene network analyses.
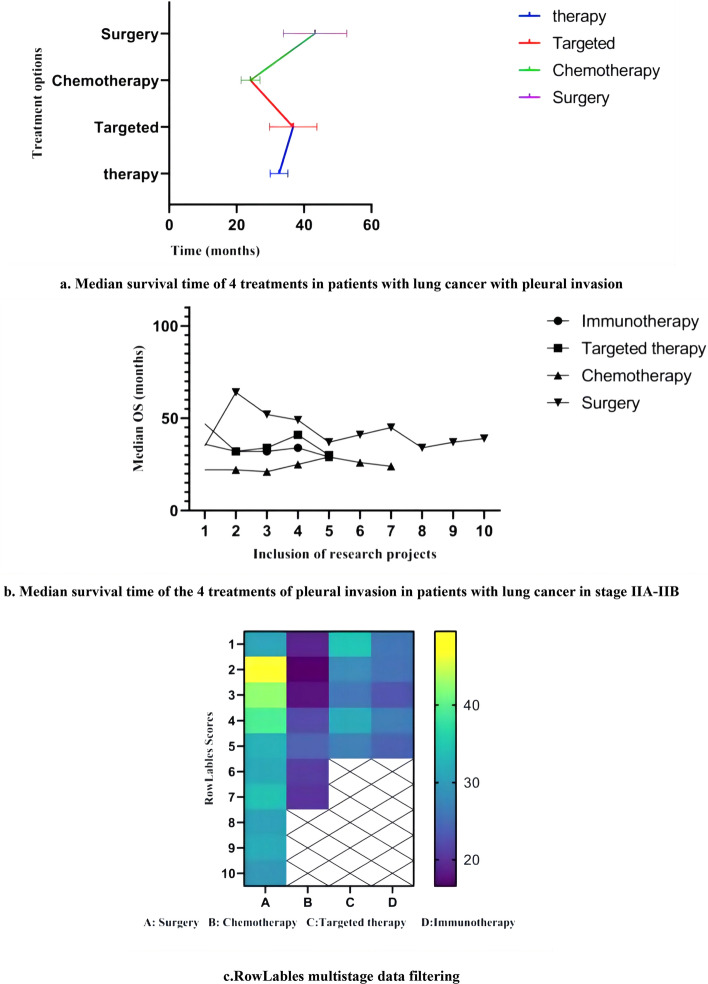
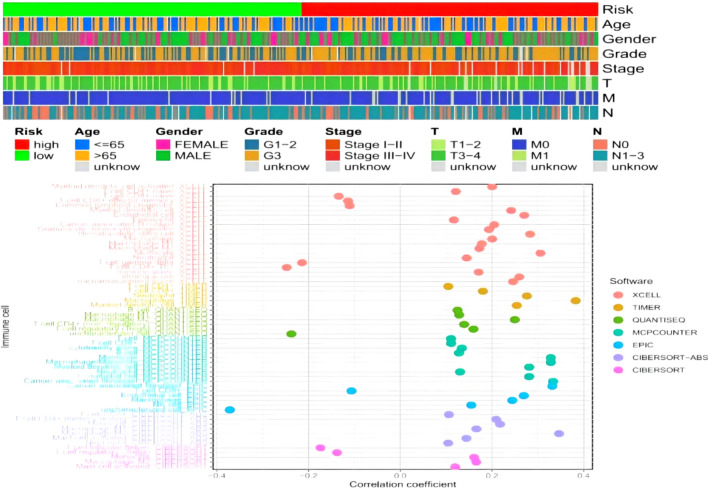
We included a total of 25 high-quality (i.e., Jadad score 4-7) studies. Meta-analysis found that surgical treatment was associated with a 3-year survival rate OR = 3.80 (95% CI 3.53, 4.09; P < 0.0001), 5-year survival rate OR = 4.10 (95% CI 3.72, 4.53; P < 0.0001), and median survival time OR = 2.71 (95% CI 2.53, 2.89; P < 0.0001). Chemotherapy was associated with a 3-year survival rate OR = 2.08 (95% CI 1.93, 2.25; P < 0.0001), 5-year survival rate OR = 1.68 (95% CI 1.49, 1.89; P < 0.0001), and median survival time OR = 1.84 (95% CI 1.66, 2.04; P < 0.0001). Targeted therapy was associated with a 3-year survival rate OR = 2.91 (95% CI 2.65, 3.19; P < 0.0001), 5-year survival rate OR = 1.83 (95% CI 1.39, 2.33; P < 0.0001), and median survival time OR = 1.76 (95% CI 1.59, 1.94; P < 0.0001). Finally, immunotherapy was associated with a 3-year survival rate OR = 1.89 (95% CI 1.73, 2.07; P < 0.0001), 5-year survival rate OR = 1.66 (95% CI 1.46, 1.88; P < 0.0001), and median survival time OR = 2.53 (95% CI 2.27, 2.82; P < 0.0001). After screening differential genes and co-expressed genes in tumor gene databases, we found that AC245595.1, ITGB1-DT and AL606489.1 may be involved in the process of lung cancer invasion, and macrophages M1 and M2, CD4+-Th1, CD8+-Th1 may participate in immune infiltration.
In patients with visceral pleural invasion of stage IIA-IIB lung cancer, chemotherapy has shown a significant effect on improving prognosis and enhancing efficacy. However, surgical treatment did not significantly improve the overall prognosis. Therefore, the individual situation of the patient and the comprehensive benefits of the treatment program should be fully considered when developing the treatment program.
肺癌脏层胸膜侵犯的治疗存在争议,尚无研究比较其四种主要治疗方案(即手术、化疗、靶向治疗和免疫治疗)的疗效。本研究旨在比较和分析手术、化疗、靶向治疗和免疫治疗的效果,并探索肺癌脏层胸膜侵犯的最佳治疗方法。
我们在电子数据库(即PubMed、Embase、Cochrane图书馆、中国知网和中国生物医学文献数据库检索)中搜索关于IIA-IIB期肺癌脏层胸膜侵犯患者治疗方案的相关研究。检索时间限制为2000年1月1日至2021年2月20日发表的研究。使用RevMan 5.3软件进行荟萃分析。我们还从GEO和TCGA肿瘤数据库下载了关于肺癌侵犯的原始RNA转录数据,并使用R 4.0.3软件进行差异表达和共表达基因网络分析。
我们共纳入25项高质量(即Jadad评分4-7)研究。荟萃分析发现,手术治疗的3年生存率OR=3.80(95%CI 3.53,4.09;P<0.0001),5年生存率OR=4.10(95%CI 3.72,4.53;P<0.0001),中位生存时间OR=2.71(95%CI 2.53,2.89;P<0.0001)。化疗的3年生存率OR=2.08(95%CI 1.93,2.25;P<0.0001),5年生存率OR=1.68(95%CI 1.49,1.89;P<0.0001),中位生存时间OR=1.84(95%CI 1.66,2.04;P<0.0001)。靶向治疗的3年生存率OR=2.91(95%CI 2.65,3.19;P<0.0001),5年生存率OR=1.83(95%CI 1.39,2.33;P<0.0001),中位生存时间OR=1.76(95%CI 1.59,1.94;P<0.0001)。最后,免疫治疗的3年生存率OR=1.89(95%CI 1.73,2.07;P<0.0001),5年生存率OR=1.66(95%CI 1.46,1.88;P<0.0001),中位生存时间OR=2.53(95%CI 2.27,2.82;P<0.0001)。在肿瘤基因数据库中筛选差异基因和共表达基因后,我们发现AC245595.1、ITGB1-DT和AL606489.1可能参与肺癌侵犯过程,巨噬细胞M1和M2、CD4+-Th1、CD8+-Th1可能参与免疫浸润。
在IIA-IIB期肺癌脏层胸膜侵犯患者中,化疗对改善预后和提高疗效显示出显著效果。然而,手术治疗并未显著改善总体预后。因此,在制定治疗方案时应充分考虑患者的个体情况和治疗方案的综合效益。