New York University Grossman School of Medicine, New York, NY, USA.
Institute for Rheumatic & Autoimmune Diseases, Atlantic Medical Group Rheumatology, Overlook Medical Center, Atlantic Health System, Summit, Morristown, NJ, NJ, USA.
Arthritis Res Ther. 2024 Sep 14;26(1):160. doi: 10.1186/s13075-024-03395-6.
The Manhattan Lupus Surveillance Program (MLSP), a population-based retrospective registry of patients with systemic lupus erythematosus (SLE), was used to investigate the prevalence of cardiovascular disease events (CVE) and compare rates among sex, age and race/ethnicity to population-based controls.
Patients with prevalent SLE in 2007 aged ≥ 20 years in the MLSP were included. CVE required documentation of a myocardial infarction or cerebrovascular accident. We calculated crude risk ratios and adjusted risk ratios (ARR) controlling for sex, age group, race and ethnicity, and years since diagnosis. Data from the 2009-2010 National Health and Nutrition Examination Survey (NHANES) and the 2013-2014 NYC Health and Nutrition Examination Survey (NYC HANES) were used to calculate expected CVE prevalence by multiplying NHANES and NYC HANES estimates by strata-specific counts of patients with SLE. Crude prevalence ratios (PRs) using national and NYC estimates and age standardized prevalence ratios (ASPRs) using national estimates were calculated.
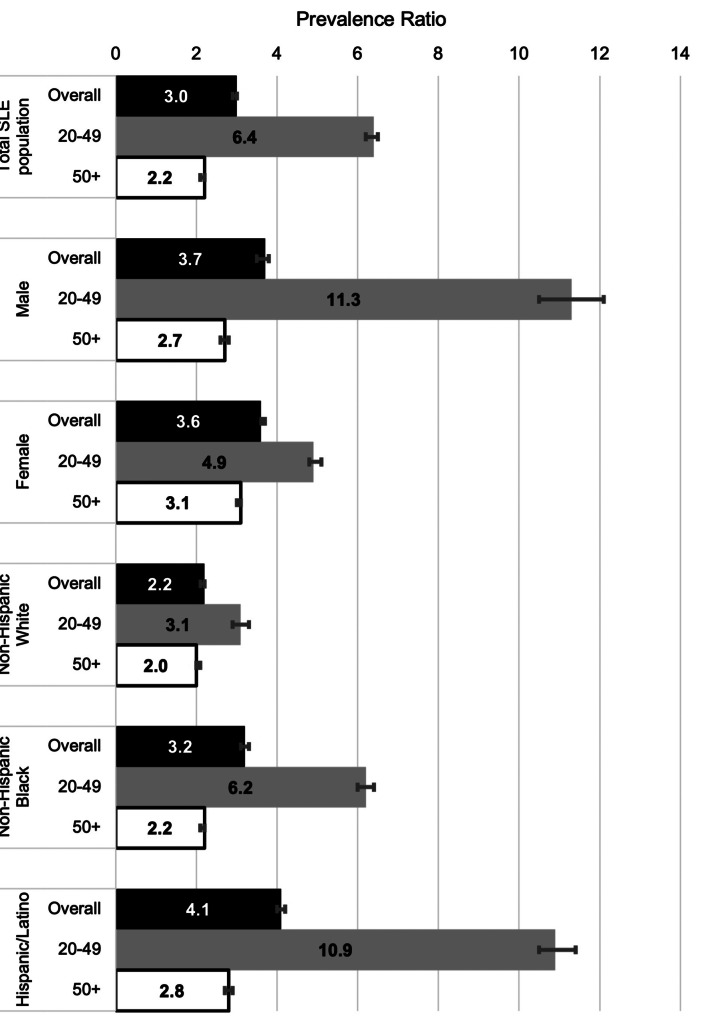
CVE occurred in 13.9% of 1,285 MLSP patients with SLE, and risk was increased among men (ARR:1.7, 95%CI:1.2-2.5) and older adults (age > 60 ARR:2.5, 95%CI:1.7-3.8). Compared with non-Hispanic Asian patients, CVE risk was elevated among Hispanic/Latino (ARR:3.1, 95%CI:1.4-7.0) and non-Hispanic Black (ARR:3.5, 95%CI1.6-7.9) patients as well as those identified as non-Hispanic and in another or multiple racial groups (ARR:4.2, 95%CI:1.1-15.8). Overall, CVE prevalence was higher among patients with SLE than nationally (ASPR:3.1, 95%CI:3.0-3.1) but did not differ by sex. Compared with national race and ethnicity-stratified estimates, CVE among patients with SLE was highest among Hispanics/Latinos (ASPR:4.3, 95%CI:4.2-4.4). CVE was also elevated among SLE registry patients compared with all NYC residents. Comparisons with age-stratified national estimates revealed PRs of 6.4 (95%CI:6.2-6.5) among patients aged 20-49 years and 2.2 (95%CI:2.1-2.2) among those ≥ 50 years. Male (11.3, 95%CI:10.5-12.1), Hispanic/Latino (10.9, 95%CI:10.5-11.4) and non-Hispanic Black (6.2, 95%CI:6.0-6.4) SLE patients aged 20-49 had the highest CVE prevalence ratios.
These population-based estimates of CVE in a diverse registry of patients with SLE revealed increased rates among younger male, Hispanic/Latino and non-Hispanic Black patients. These findings reinforce the need to appropriately screen for CVD among all SLE patients but particularly among these high-risk patients.
曼哈顿狼疮监测计划(MLSP)是一个基于人群的系统性红斑狼疮(SLE)患者回顾性登记处,用于调查心血管疾病事件(CVE)的患病率,并比较不同性别、年龄和种族/族裔的发生率与基于人群的对照。
纳入 2007 年 MLSP 中年龄≥20 岁的现患 SLE 患者。CVE 需要心肌梗死或脑血管意外的记录。我们计算了粗风险比和调整后的风险比(ARR),控制了性别、年龄组、种族和族裔以及诊断后年限。使用 2009-2010 年全国健康和营养检查调查(NHANES)和 2013-2014 年纽约市健康和营养检查调查(NYC HANES)的数据,通过将 NHANES 和 NYC HANES 估计值乘以患者 SLE 的特定分层计数来计算预期的 CVE 患病率。使用全国和 NYC 估计值计算粗患病率比(PR),使用全国估计值计算年龄标准化患病率比(ASPR)。
1285 例 MLSP 患者中发生了 13.9%的 CVE,男性(ARR:1.7,95%CI:1.2-2.5)和老年人(年龄>60 ARR:2.5,95%CI:1.7-3.8)的风险增加。与非西班牙裔亚洲患者相比,西班牙裔/拉丁裔(ARR:3.1,95%CI:1.4-7.0)和非西班牙裔黑种人(ARR:3.5,95%CI 1.6-7.9)患者以及被确定为非西班牙裔且属于另一个或多个种族群体的患者(ARR:4.2,95%CI:1.1-15.8)的 CVE 风险更高。总体而言,SLE 患者的 CVE 患病率高于全国(ASPR:3.1,95%CI:3.0-3.1),但性别差异无统计学意义。与全国种族和族裔分层估计值相比,SLE 患者的 CVE 发生率在西班牙裔/拉丁裔中最高(ASPR:4.3,95%CI:4.2-4.4)。与所有纽约市居民相比,SLE 登记患者的 CVE 也有所增加。与年龄分层的全国估计值相比,20-49 岁患者的 PR 为 6.4(95%CI:6.2-6.5),≥50 岁患者的 PR 为 2.2(95%CI:2.1-2.2)。男性(11.3,95%CI:10.5-12.1)、西班牙裔/拉丁裔(10.9,95%CI:10.5-11.4)和非西班牙裔黑种人(6.2,95%CI:6.0-6.4)的 20-49 岁 SLE 患者的 CVE 患病率比最高。
这些基于人群的 SLE 患者 CVD 发生率的估计值显示,年轻男性、西班牙裔/拉丁裔和非西班牙裔黑种人患者的发生率较高。这些发现强调了需要对所有 SLE 患者进行适当的 CVD 筛查,但特别是对这些高危患者进行筛查。