Maugeri Rosario, Bonosi Lapo, Brunasso Lara, Costanzo Roberta, Santi Samuele, Signorelli Francesco, Iacopino Domenico Gerardo, Visocchi Massimiliano
Neurosurgical Clinic, AOUP "Paolo Giaccone", Post Graduate Residency Program in Neurologic Surgery, Department of Experimental Biomedicine and Clinical Neurosciences, School of Medicine, University of Palermo, Via del Vespro 127, 90127 Palermo, Italy.
Department of Neurosurgery, Fondazione Policlinico Agostino Gemelli IRCCS, Largo Agostino Gemelli 8, 00168 Rome, Italy.
J Clin Med. 2024 Aug 26;13(17):5052. doi: 10.3390/jcm13175052.
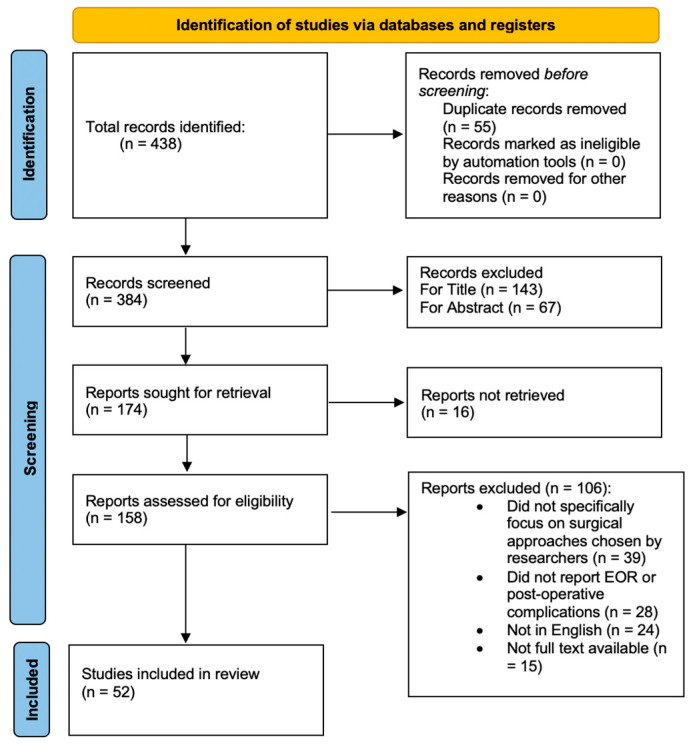
Clival chordomas represent a rare but clinically significant subset of skull base tumors, characterized by a locally aggressive nature and a location in proximity to vital neurovascular structures. Surgical resection, often combined with adjuvant therapies, remains the cornerstone of clival chordoma treatment, and various approaches and techniques have evolved to maximize tumor removal while preserving neurological function. Recent advancements in skull base surgery, imaging, and adjuvant therapies have improved outcomes by reducing morbidity and thus enhancing long-term survival. We have conducted a systematic review on PubMed/Medline following PRISMA guidelines regarding indications, the extent of resection (EOR), and complication rates. Then, we present three illustrative cases from our personal experience, which started 25 years ago with CVJ instrumentation procedures and 15 years ago with anterior decompressive transmucosal procedures performed with the aid of an operative microscope, an endoscope, and neuroradiological monitoring. Traditionally, the transoral approach (TOA) is the most frequently used corridor for accessing the lower clivus and the anterior craniovertebral junction (CVJ), without the need to mobilize or retract neural structures; however, it is associated with a high rate of complications. The endonasal approach (EEA) provides access to the anterior CVJ as well as to the lower, middle, and superior clivus, decreasing airway and swallowing morbidity, preserving palatal function, decreasing postoperative pain, and reducing the incidence of tracheostomy. The submandibular retropharyngeal approach (SRA) allows unique access to certain cervical chordomas, which is better suited when the lesion is located below the clivus and in the midline.
斜坡脊索瘤是一种罕见但具有临床意义的颅底肿瘤亚型,其特点是具有局部侵袭性,且位于重要神经血管结构附近。手术切除通常联合辅助治疗,仍然是斜坡脊索瘤治疗的基石,并且已经发展出各种方法和技术,以在保留神经功能的同时最大限度地切除肿瘤。颅底手术、影像学和辅助治疗方面的最新进展通过降低发病率从而提高了长期生存率,改善了治疗效果。我们按照PRISMA指南在PubMed/Medline上对有关适应症、切除范围(EOR)和并发症发生率进行了系统综述。然后,我们介绍了来自我们个人经验的三个典型病例,这些病例始于25年前的颅颈交界区(CVJ)器械操作程序,以及15年前借助手术显微镜、内窥镜和神经放射学监测进行的前路减压经粘膜手术。传统上,经口入路(TOA)是进入下斜坡和前颅颈交界区(CVJ)最常用的通道,无需移动或牵拉神经结构;然而,它与高并发症发生率相关。鼻内镜入路(EEA)可进入前颅颈交界区以及下、中、上斜坡,降低气道和吞咽并发症,保留腭功能,减轻术后疼痛,并降低气管切开术的发生率。下颌下咽后入路(SRA)可独特地进入某些颈椎脊索瘤,当病变位于斜坡下方且在中线时更适用。