Muto Jun, Tateya Ichiro, Nakatomi Hirofumi, Uyama Ichiro, Hirose Yuichi
Department of Neurosurgery, Fujita Health University, Aichi, Japan.
Department of Otolaryngology-Head and Neck Surgery, Fujita Health University, Aichi, Japan.
Neurospine. 2024 Mar;21(1):106-115. doi: 10.14245/ns.2448062.031. Epub 2024 Mar 31.
The application of the da Vinci Surgical System in neurosurgery is limited due to technical difficulties requiring precise maneuvers and small instruments. This study details the advantages and disadvantages of robotics in neurosurgery and the reachable range of the transoral approach to lesions of the skull base and upper cervical spine.
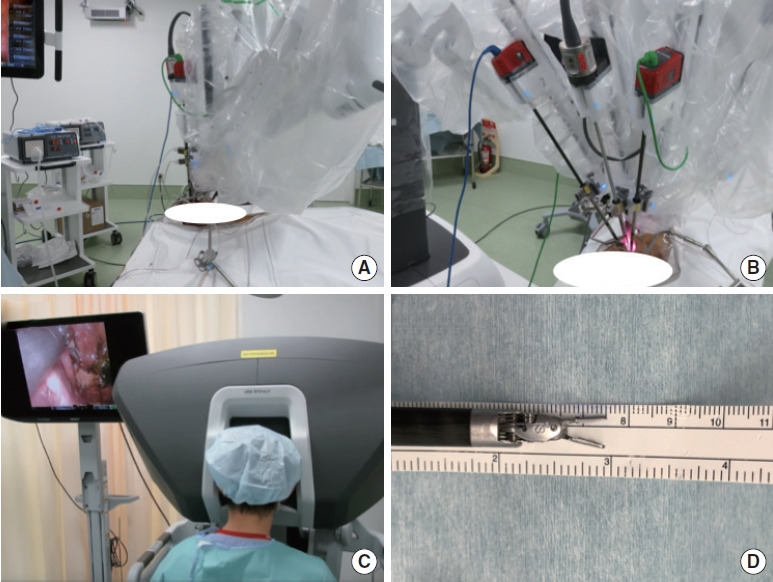
In a cadaver study, the da Vinci Xi robot, lacking haptic feedback, was utilized for sagittal and coronal approaches on 5 heads, facilitating dura suturing in 3, with a 30°-angled drill for bone removal.
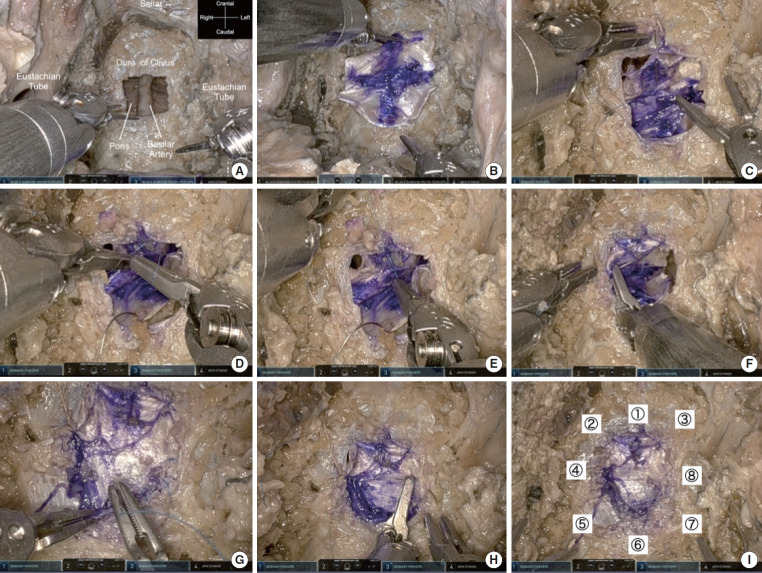
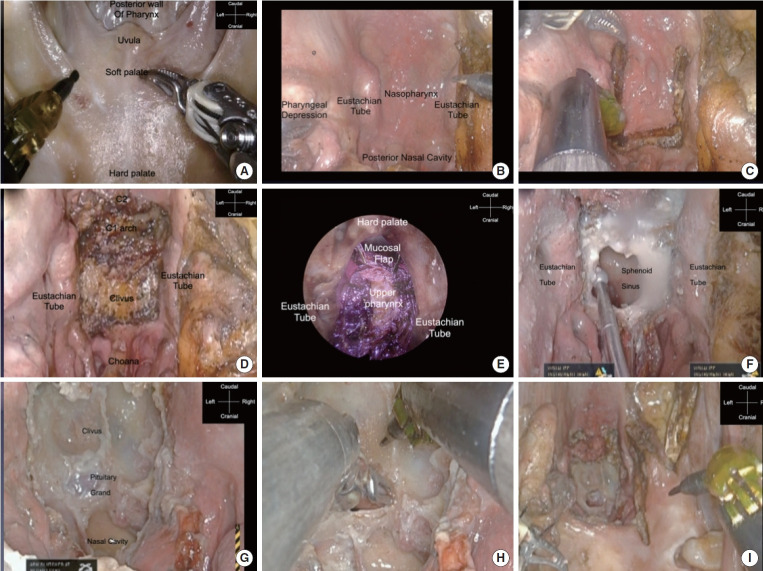
Perfect exposure of all the nasopharyngeal sites, clivus, sellar, and choana, including the bilateral eustachian tubes, was achieved without any external incisions using this palatal split approach of transoral robotic surgery. The time required to perform a single stitch, knot, and complete single suture in robotic suturing of deep-seated were significantly less compared to manual suturing via the endonasal approach.
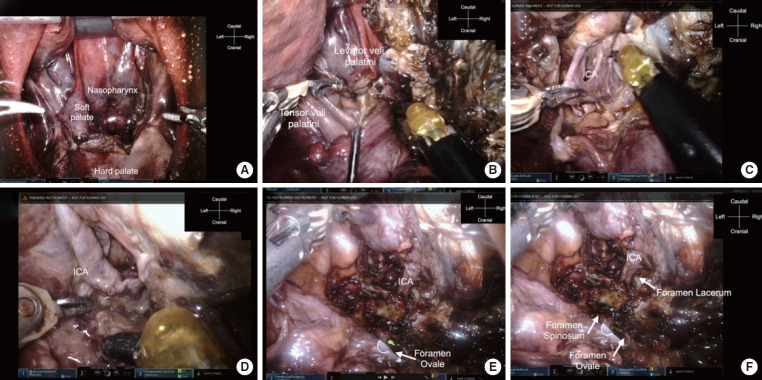
This is the first report to show the feasibility of suturing the dural defect in deep-seated lesions transorally and revealed that the limit of reach in the coronal plane via a transoral approach with incision of the soft palate is the foramen ovale. This preclinical investigation also showed that the transoral robotic approach is feasible for lesions extending from the sellar to the C2 in the sagittal plane. Refinement of robotic instruments for specific anatomic sites and future neurosurgical studies are needed to further demonstrate the feasibility and effectiveness of this system in treating benign and malignant skull base lesions.
由于达芬奇手术系统在神经外科手术中应用时存在技术难题,需要精确操作且器械细小,其应用受到限制。本研究详细阐述了机器人技术在神经外科手术中的优缺点,以及经口入路治疗颅底和上颈椎病变的可达范围。
在一项尸体研究中,使用缺乏触觉反馈的达芬奇Xi机器人对5个头部进行矢状位和冠状位入路手术,其中3例辅助进行硬脑膜缝合,使用30°角钻头进行骨切除。
采用经口机器人手术的腭部劈开入路,无需任何外部切口,即可完美暴露所有鼻咽部、斜坡、鞍区和后鼻孔,包括双侧咽鼓管。与经鼻入路手动缝合相比,机器人缝合深部组织时单针、打结和完成单缝所需时间显著减少。
这是首份展示经口缝合深部病变硬脑膜缺损可行性的报告,揭示了经口软腭切开入路在冠状面的可达极限是卵圆孔。这项临床前研究还表明,经口机器人入路在矢状面治疗从鞍区延伸至C2的病变是可行的。需要针对特定解剖部位改进机器人器械,并开展未来的神经外科研究,以进一步证明该系统在治疗颅底良恶性病变方面的可行性和有效性。