Wisanumahimachai Veera, Pongsatha Saipin, Chatchawarat Latchee, Tongsong Theera
Department of Obstetrics and Gynecology, Faculty of Medicine, Chiang Mai University, Chiang Mai 50200, Thailand.
J Clin Med. 2024 Sep 9;13(17):5332. doi: 10.3390/jcm13175332.
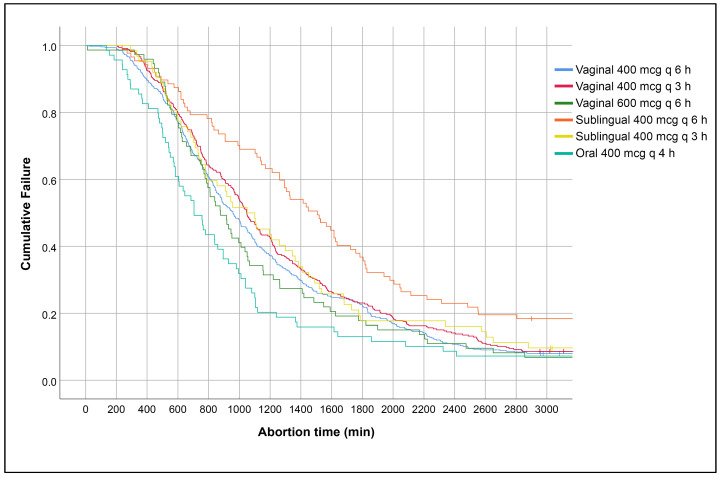
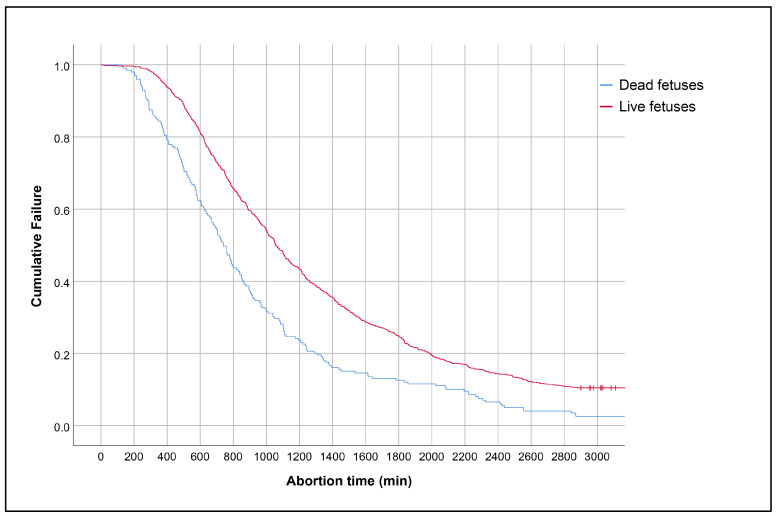
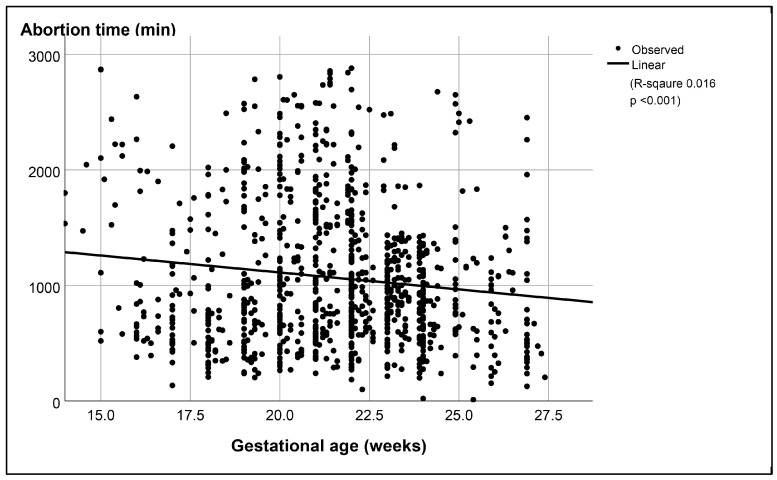
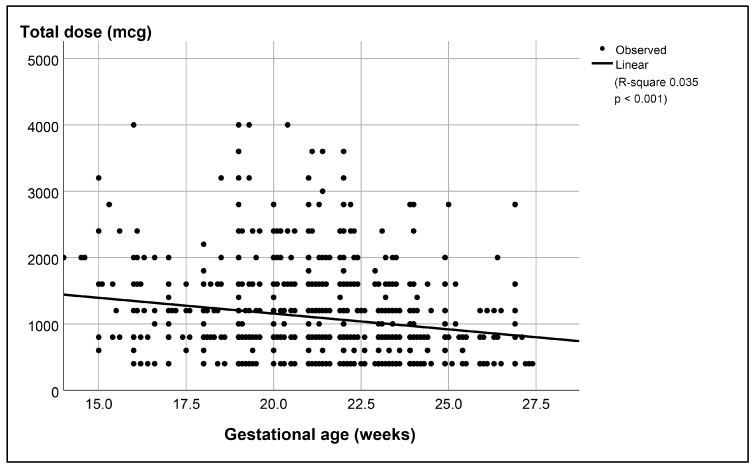
Understanding the potential risk factors for failure of pregnancy termination is crucial for informed clinical decision making. Such insights can assist clinicians in adjusting the dosage or route of various regimens, as well as in counseling patients and predicting the likelihood of successful outcomes. However, research on these risk factors has been limited, and existing studies have yielded inconsistent results. To address this gap, we conducted a study with a large sample size, focusing on identifying the potential risk factors for failure of second-trimester termination using misoprostol as a single agent, specifically between 14 and 28 weeks of gestation. A secondary analysis based on a database of second-trimester terminations was conducted. The inclusion criteria were a singleton pregnancy, gestational age between 14 and 28 weeks, an unfavorable cervix, no spontaneous labor pain, intact membranes, and termination with misoprostol alone. Potential risk factors for failure of termination, defined as no abortion within 48 h, were analyzed using univariate and multivariate analyses. A total of 1094 cases were included in the analysis, consisting of 991 successful cases and 103 (9.4%) cases of failure. The significant risk factors for failure of termination included early gestational age, live fetuses, sublingual regimen of 400 mcg every 6 h, and high maternal pre-pregnancy BMI. Previous cesarean sections and lower Bishop scores tended to increase the risk but did not reach a significant level. Second-trimester termination with misoprostol as a single agent was highly effective, with a failure rate of 9.4%. The risk factors for failure included gestational age, fetal viability, misoprostol regimen, and maternal pre-pregnancy BMI, suggesting that these factors should be taken into consideration for second-trimester terminations with misoprostol.
了解妊娠终止失败的潜在风险因素对于做出明智的临床决策至关重要。这些见解有助于临床医生调整各种治疗方案的剂量或给药途径,以及为患者提供咨询并预测成功结局的可能性。然而,关于这些风险因素的研究有限,现有研究结果也不一致。为了填补这一空白,我们进行了一项大样本研究,重点是确定使用米索前列醇作为单一药物进行孕中期终止(具体为妊娠14至28周之间)失败的潜在风险因素。我们基于一个孕中期终止数据库进行了二次分析。纳入标准为单胎妊娠、孕龄在14至28周之间、宫颈条件不佳、无自发宫缩痛、胎膜完整且仅使用米索前列醇进行终止妊娠。将终止失败定义为48小时内未流产,使用单因素和多因素分析来分析终止失败的潜在风险因素。共有1094例病例纳入分析,其中991例成功,103例(9.4%)失败。终止失败的显著风险因素包括孕龄小、活胎、每6小时舌下含服400微克的给药方案以及孕前较高的孕妇体重指数。既往剖宫产史和较低的 Bishop 评分倾向于增加风险,但未达到显著水平。以米索前列醇作为单一药物进行孕中期终止妊娠非常有效,失败率为9.4%。失败的风险因素包括孕龄、胎儿活力、米索前列醇给药方案和孕前孕妇体重指数,这表明在使用米索前列醇进行孕中期终止妊娠时应考虑这些因素。