Mishra Ajay Kumar, Mateen Saboor, Jabeen Firdaus, Singh Shivesh, Verma Pankaj Kumar
Department of Medicine, Era's Lucknow Medical College and Hospital, Lucknow, Uttar Pradesh, India.
Ochsner J. 2024 Fall;24(3):219-224. doi: 10.31486/toj.24.0019.
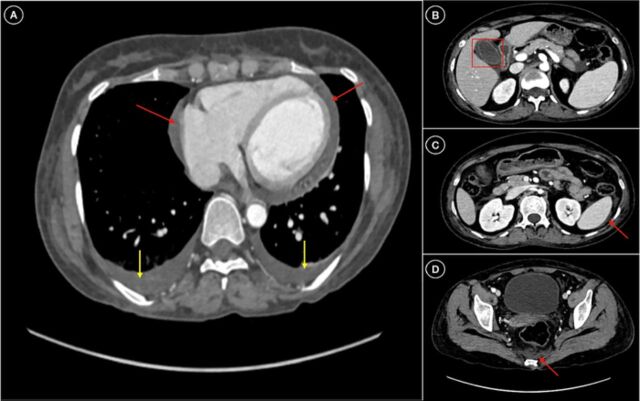
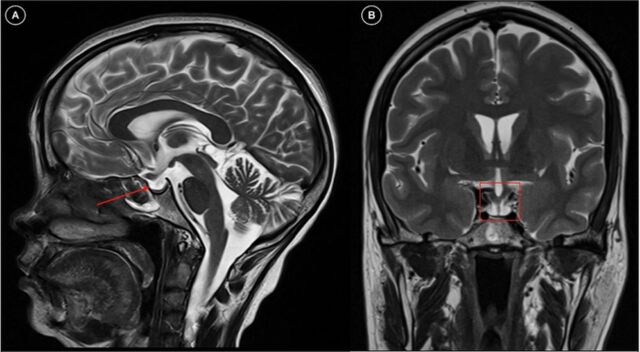
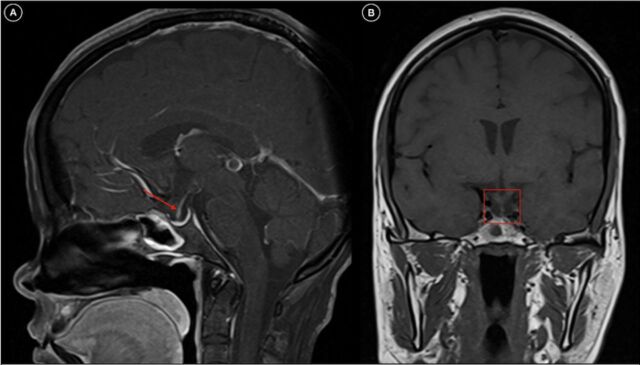
Sheehan syndrome is the infarction of a pituitary gland that has been physiologically enlarged as a result of postpartum bleeding. Agalactorrhea and amenorrhea are classic symptoms, but a constellation of manifestations occurs in both the acute and chronic forms. These manifestations can remain largely nonemergent unless Sheehan syndrome is complicated by severe adrenal dysfunction secondary to an inciting event such as dengue. We present a case of Sheehan syndrome that was uncovered in a patient with a dengue infection presenting as adrenal crisis. A 45-year-old female presented with symptoms of acute gastroenteritis and severe dehydration. Her medical history was significant for secondary amenorrhea for 14 years after her last delivery followed by symptoms of endocrine dysfunction. At presentation, the patient was in adrenal crisis with hypotension, hypoglycemia, and hyperthermia. Dengue nonstructural protein 1 antigen was positive, along with signs of plasma leakage. Bloodwork showed bicytopenia with abnormal liver enzymes. Ultrasonography and computed tomography of the abdomen were suggestive of serositis with acalculous cholecystitis. Magnetic resonance imaging of the brain revealed an empty sella. Anterior pituitary hormone levels were significantly decreased with low serum cortisol, and the patient's thyroid profile analysis suggested secondary hypothyroidism. The final diagnosis was Sheehan syndrome presenting as adrenal crisis precipitated by severe dengue fever. The patient was managed conservatively and discharged on hormone supplement therapy. Sheehan syndrome is an important cause of panhypopituitarism in the developing world. Knowledge of Sheehan syndrome is important to help prevent its occurrence and reduce its resultant multifactorial effects.
席汉综合征是由于产后出血导致生理性增大的垂体发生梗死。无乳和闭经是典型症状,但急性和慢性形式均会出现一系列表现。这些表现大多不会很紧急,除非席汉综合征因登革热等诱发事件并发严重肾上腺功能不全。我们报告一例在因登革热感染表现为肾上腺危象的患者中发现的席汉综合征病例。一名45岁女性出现急性胃肠炎和严重脱水症状。她的病史显示,末次分娩后继发闭经14年,随后出现内分泌功能障碍症状。就诊时,患者处于肾上腺危象状态,伴有低血压、低血糖和高热。登革热非结构蛋白1抗原呈阳性,伴有血浆渗漏迹象。血液检查显示全血细胞减少伴肝酶异常。腹部超声和计算机断层扫描提示浆膜炎伴无结石性胆囊炎。脑部磁共振成像显示空蝶鞍。垂体前叶激素水平显著降低,血清皮质醇水平低,患者的甲状腺功能分析提示继发性甲状腺功能减退。最终诊断为席汉综合征,表现为严重登革热引发的肾上腺危象。患者接受保守治疗,出院时接受激素补充治疗。席汉综合征是发展中国家全垂体功能减退的重要原因。了解席汉综合征对于预防其发生和减少其产生的多因素影响很重要。