Cione Ferdinando, De Bernardo Maddalena, Di Paola Ilenia, Caputo Alessandro, Graziano Mario, Rosa Nicola
Ophthalmological Unit, Department of Medicine, Surgery and Dentistry, Scuola Medica Salernitana, University of Salerno, Salerno, Italy.
AOU San Giovanni di Dio e Ruggi D'Aragona, Salerno, Italy.
Heliyon. 2024 Aug 23;10(17):e36609. doi: 10.1016/j.heliyon.2024.e36609. eCollection 2024 Sep 15.
Comparing IOL power calculation formulas in long eyes (AL≥26.00 mm) to find the best axial length (AL) adjustment/IOL power calculation formula combination.
Retrospective, comparative, case-series.
Patients with long eyes that underwent cataract surgery.
five-hundred-fifty-four eyes of 554 patients were examined before and after standard phacoemulsification without complications. Eyes were subdivided in 3 groups according to AL: 26.00≤AL<28.00 mm, 28.00≤AL<30.00 mm, AL≥30.00 mm. Eight formulas that do not require anterior chamber depth (ACD) were evaluated: Barrett Universal II (BUII), Emmetropia Verifying Optical (EVO) 2.0, Ladas Super Formula (LSF), Hoffer Q, Holladay 1, SRKT, T2 and T2.2. The lens constant of ULIB database and IOLCon database were used. Each formula was analyzed by using uncorrected AL (ALu) and following AL adjustments: Wang-Koch 1 (wk1), wk2, wk polinomial (wk-pol), estimated Cooke modified axial length (CMALe) and ALc correcting factor.
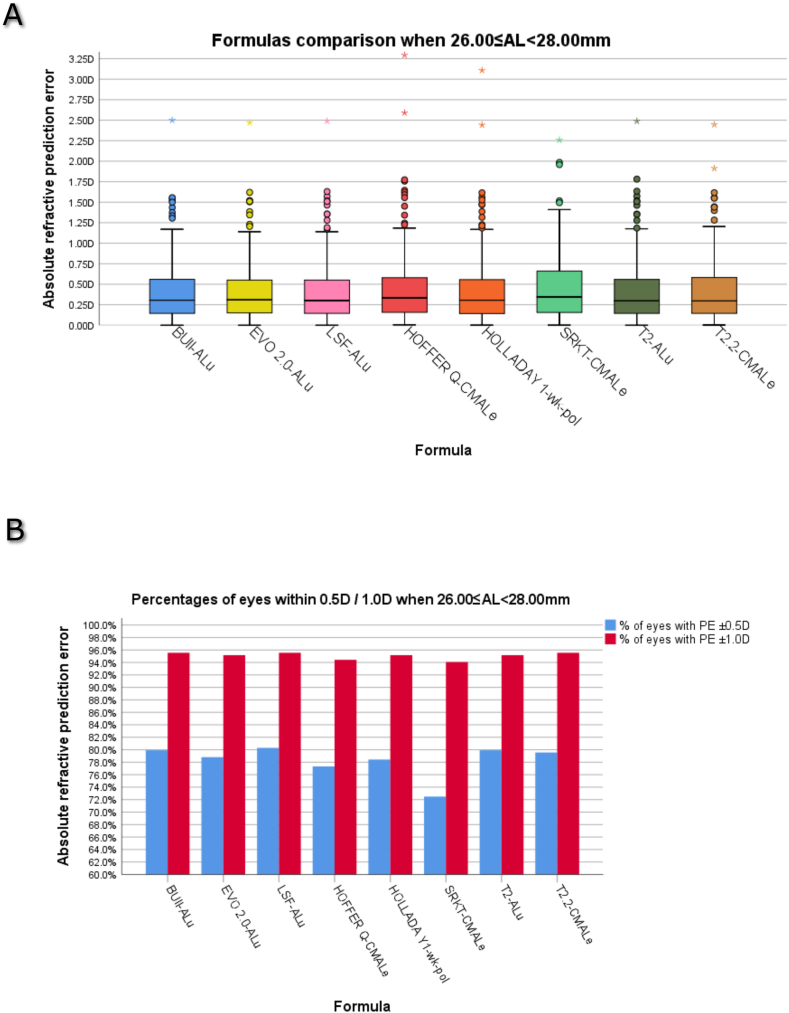
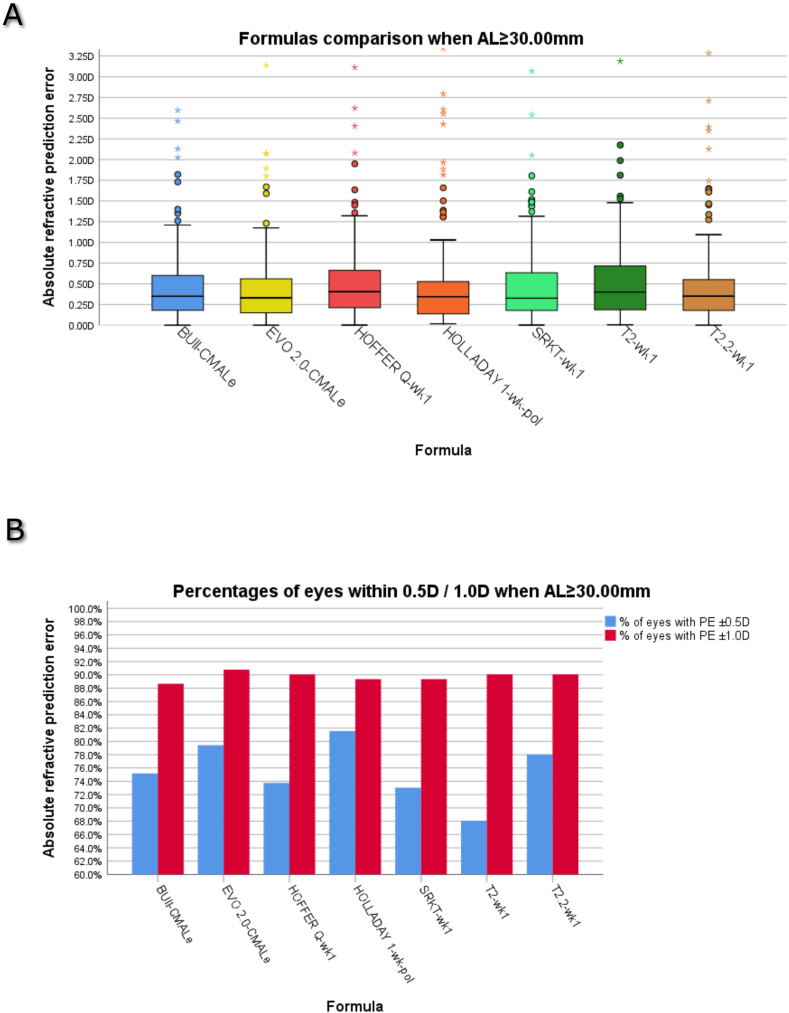
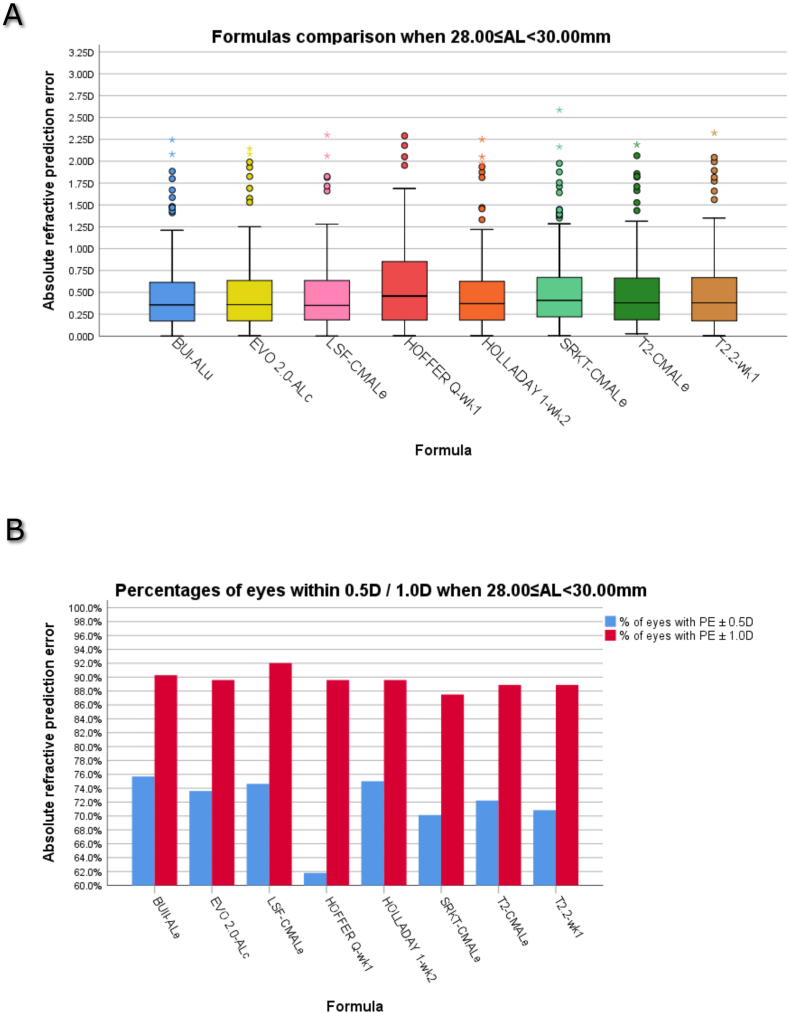
Mean absolute error (MAE), median absolute error (MedAE) and percentage of eyes within ±0.50 and ± 1.00 diopters (D) of prediction error.
T2-ALu gave best outcome when 26.00 mm ≤ AL<28.00 mm. LSF-ALu, BUII-ALu, EVO 2.0-ALu, Holladay 1-wk-pol and T2.2-CMALe represented valid alternatives. EVO 2.0-ALc gave best outcomes when 28.00 mm ≤ AL<30.00 mm. Other thick-lens or hybrid artificial-intelligence-vergence based formulas (BUII-ALu, LSF-CMALe) and Holladay 1-wk2 demonstrated greater reliability compared to thin lens-based formulas. EVO 2.0-CMALe gave best outcomes when AL≥30.00 mm. Holladay 1-wk-pol e T2.2-wk1 represented valid alternatives (all p < 0.050). LSF could fail in 50 % of cases without ACD when AL≥30.00 mm.
Choosing the best AL adjustment/IOL power calculation formula combination for each AL subrange, can improve refractive outcomes in patients with long eyes that undergo cataract surgery.
比较长眼(眼轴长度[AL]≥26.00mm)的人工晶状体(IOL)屈光度计算公式,以找出最佳的眼轴长度调整/IOL屈光度计算公式组合。
回顾性、对比性病例系列研究。
接受白内障手术的长眼患者。
对554例患者的554只眼在标准超声乳化手术前后进行检查,且无并发症。根据眼轴长度将眼分为3组:26.00≤AL<28.00mm、28.00≤AL<30.00mm、AL≥30.00mm。评估了8种无需前房深度(ACD)的公式:巴雷特通用二代(BUII)、正视验证光学(EVO)2.0、拉达斯超级公式(LSF)、霍弗Q公式、霍拉迪1公式、SRKT公式、T2公式和T2.2公式。使用了ULIB数据库和IOLCon数据库的晶状体常数。每个公式通过使用未校正的眼轴长度(ALu)以及以下眼轴长度调整进行分析:王-科赫1(wk1)、wk2、wk多项式(wk-pol)、估计的库克修正眼轴长度(CMALe)和ALc校正因子。
平均绝对误差(MAE)、中位数绝对误差(MedAE)以及预测误差在±0.50和±1.00屈光度(D)范围内的眼的百分比。
当26.00mm≤AL<28.00mm时,T2-ALu得出最佳结果。LSF-ALu、BUII-ALu、EVO 2.0-ALu、霍拉迪1-wk-pol和T2.2-CMALe是有效的替代方案。当28.00mm≤AL<30.00mm时EVO 2.0-ALc得出最佳结果。与基于薄透镜的公式相比,其他基于厚透镜或混合人工智能聚散度的公式(BUII-ALu、LSF-CMALe)和霍拉迪1-wk2显示出更高的可靠性。当AL≥30.00mm时,EVO 2.0-CMALe得出最佳结果。霍拉迪1-wk-pol和T2.2-wk1是有效的替代方案(所有p<0.050)。当AL≥30.00mm时,如果没有前房深度数据,LSF在50%的病例中可能会失败。
为每个眼轴长度子范围选择最佳的眼轴长度调整/IOL屈光度计算公式组合,可以改善接受白内障手术的长眼患者的屈光效果。