Poghosyan Hermine, Sarkar Sayantani, Richman Ilana, Pietrzak Robert H, Carter-Bawa Lisa, Cooley Mary E
Yale School of Nursing, Yale University, New Haven, Connecticut.
Cancer Outcomes, Public Policy, and Effectiveness Research (COPPER) Center, Yale School of Medicine, New Haven, Connecticut.
JTO Clin Res Rep. 2024 Jul 6;5(9):100705. doi: 10.1016/j.jtocrr.2024.100705. eCollection 2024 Sep.
Although COVID-19 has affected health care and screening utilization, its impact on lung cancer screening (LCS) uptake remains unclear. Our study investigated LCS utilization and associated predictors among adults eligible for LCS before (2019), during (2020-2021), and at a later stage (2022) of COVID-19.
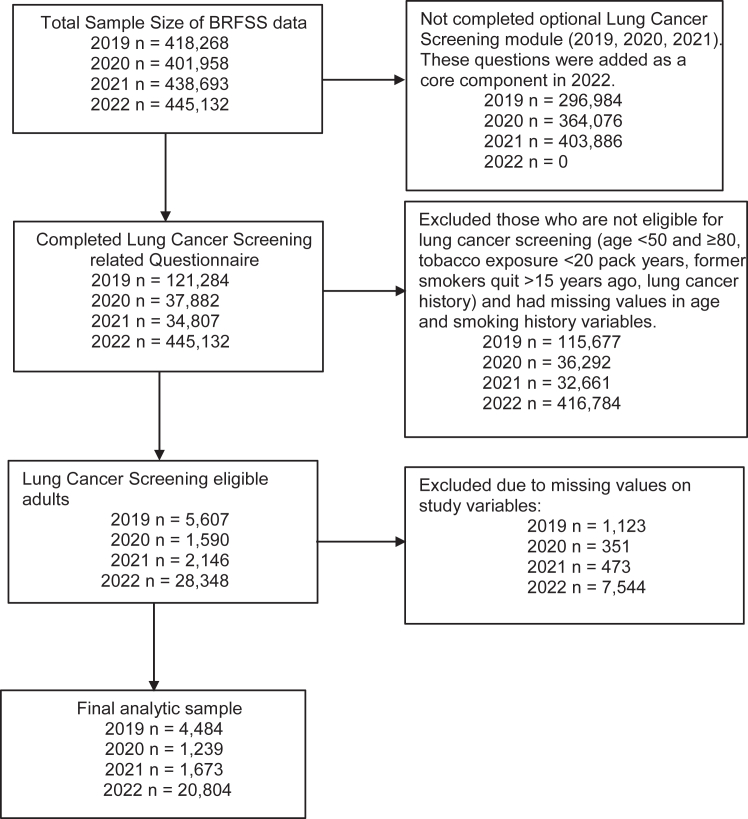
We used cross-sectional, nationally representative, population-based data from the Behavioral Risk Factor Surveillance System over 4 consecutive years: 2019 (n = 4484; weighted n = 1,559,37), 2020 (n = 1239; weighted n = 200,301), 2021 (n = 1673; weighted n = 668,359), and 2022 (n = 20,804; weighted n = 9,458,907). The outcome was self-reported LCS uptake (0 = did not have LCS in the past 12 mo and 1 = underwent LCS in the past 12 mo). We conducted weighted statistics and multivariable logistic regression.
Overall, of 11,886,704 million individuals eligible for LCS, 2,129,900 received LCS in 4 years (2019-2022). National rates of LCS among individuals eligible for screening were 16.3% (95% confidence interval [CI]:14.4-18.5), 19.4% (95% CI:15.3-24.3), 18.3% (95% CI:15.6-21.3), and 18.1% (95% CI:17.1-19.2) in 2019, 2020, 2021, and 2022, respectively. Respondents reporting lung disease and cancer (other than lung cancer) history were more likely to receive LCS across all 4 years. During the pandemic (2020), Hispanic (versus White), and rural (versus urban) residents had lower odds of LCS utilization. In 2022, men had increased odds of reporting LCS use relative to women. No sex differences in LCS use were observed in previous years.
Our findings indicate consistently low LCS utilization (<20%) over 4 years. Nationwide efforts to boost LCS awareness and utilization are essential for mitigating the lung cancer burden in the United States.
尽管新冠疫情影响了医疗保健和筛查的使用情况,但其对肺癌筛查(LCS)接受率的影响仍不明确。我们的研究调查了在新冠疫情之前(2019年)、期间(2020 - 2021年)以及后期(2022年)符合肺癌筛查条件的成年人的肺癌筛查使用情况及相关预测因素。
我们使用了行为风险因素监测系统连续4年的横断面、具有全国代表性的基于人群的数据:2019年(n = 4484;加权n = 1,559,37)、2020年(n = 1239;加权n = 200,301)、2021年(n = 1673;加权n = 668,359)和2022年(n = 20,804;加权n = 9,458,907)。结果变量是自我报告的肺癌筛查接受情况(0 = 在过去12个月内未进行肺癌筛查,1 = 在过去12个月内接受了肺癌筛查)。我们进行了加权统计和多变量逻辑回归分析。
总体而言,在11,886,704名符合肺癌筛查条件的个体中,有2,129,900人在4年(2019 - 2022年)内接受了肺癌筛查。在符合筛查条件的个体中,2019年、2020年、2021年和2022年的全国肺癌筛查率分别为16.3%(95%置信区间[CI]:14.4 - 18.5)、19.4%(95% CI:15.3 - 24.3)、18.3%(95% CI:15.6 - 21.3)和18.1%(95% CI:17.1 - 19.2)。在所有4年中,报告有肺部疾病和癌症(非肺癌)病史的受访者更有可能接受肺癌筛查。在疫情期间(2020年),西班牙裔(与白人相比)和农村居民(与城市居民相比)接受肺癌筛查的几率较低。2022年,男性报告接受肺癌筛查的几率相对于女性有所增加。在之前几年中未观察到肺癌筛查使用方面的性别差异。
我们的研究结果表明,在4年期间肺癌筛查的使用率一直较低(<20%)。在美国,全国范围内提高肺癌筛查意识和使用率的努力对于减轻肺癌负担至关重要。