Davis Ryan, Ladbury Colton, Tsai Kevin, Maraghechi Borna, Shi Chengyu, Li Rose, Glaser Scott, Dandapani Savita, Wong Jeffrey, Williams Terence, Lee Percy
Radiation Oncology, City of Hope National Medical Center, Duarte, USA.
Radiation Oncology, City of Hope Orange County Lennar Foundation Cancer Center, Irvine, USA.
Cureus. 2024 Aug 20;16(8):e67318. doi: 10.7759/cureus.67318. eCollection 2024 Aug.
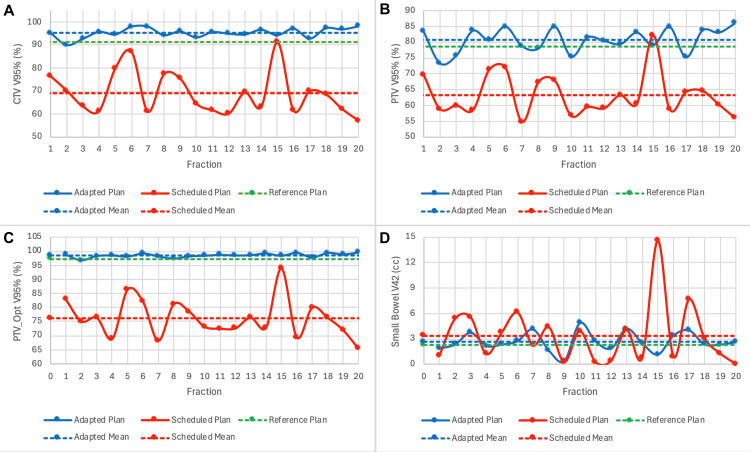
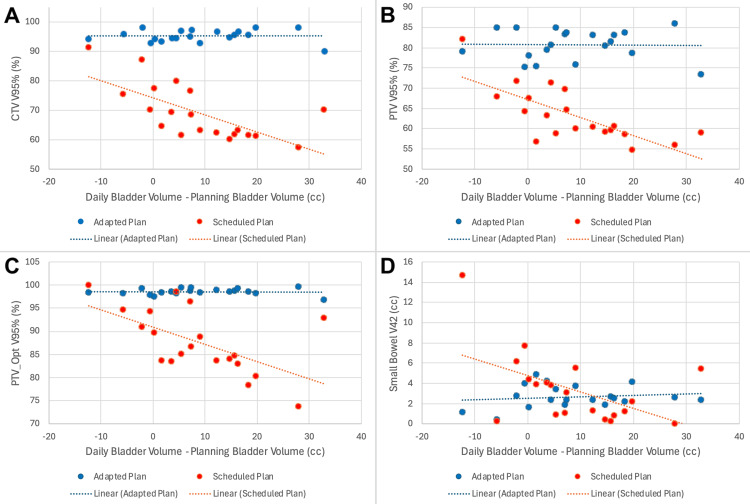
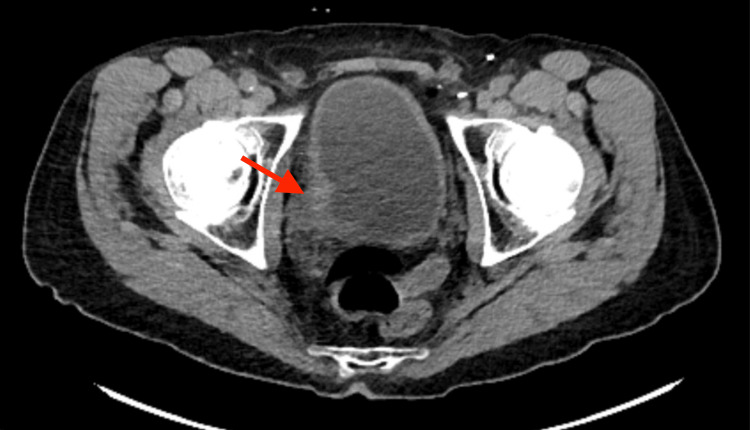
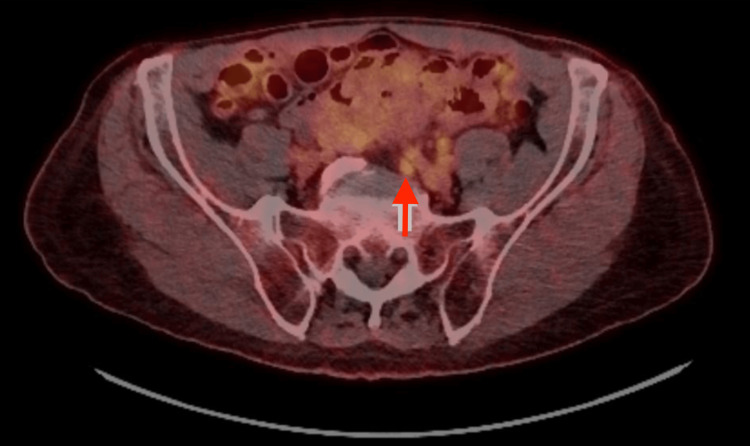
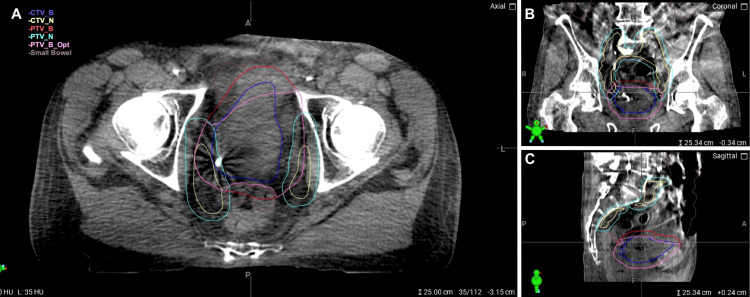
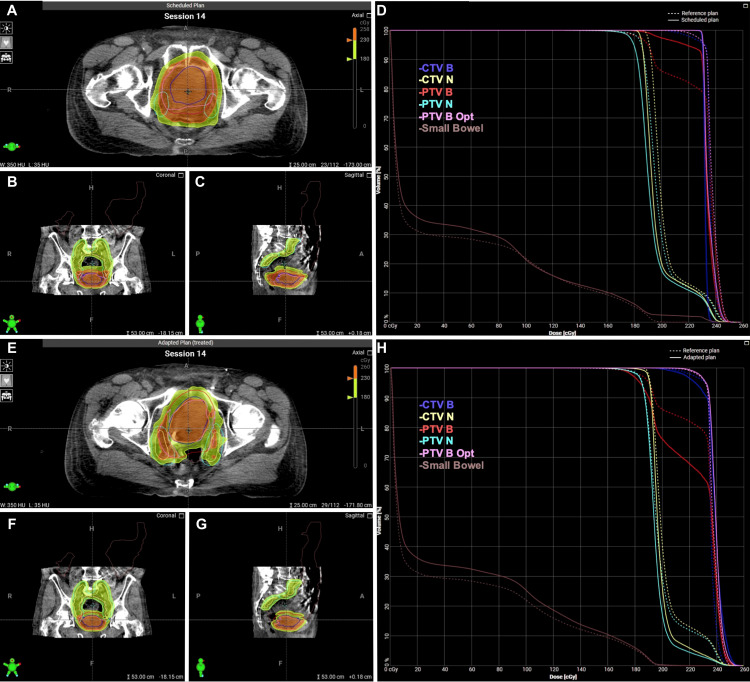
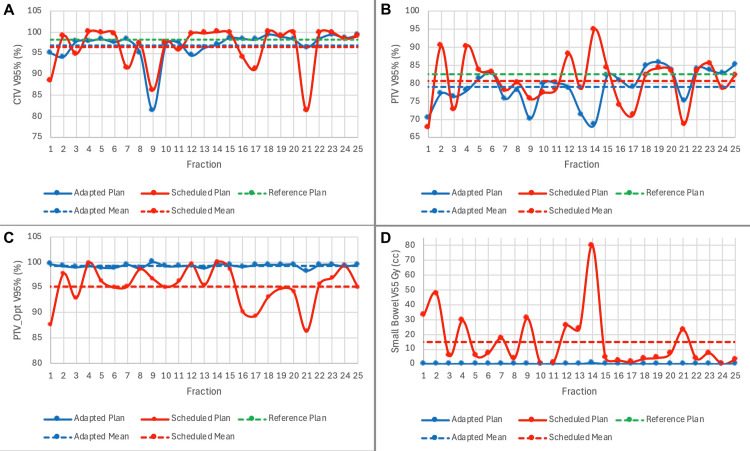
Trimodality treatment for bladder cancer, consisting of maximal transurethral resection of the tumor followed by concurrent chemoradiotherapy, is an attractive management option with curative and organ-sparing intent. However, such treatment can be associated with acute toxicities related to the large treatment margins required due to daily variation in bladder filling, with resultant bladder, bowel, and rectal toxicity. Adaptive radiation, which accounts for inter-fraction variations in bladder size, allows the confident delivery of radiation to bladder cancer with smaller margins, with the potential to reduce toxicities without the associated risk of compromising the target coverage. Herein, we present a case series of two patients with primary bladder cancer who were treated with computed tomography (CT)-based online adaptive hypofractionated radiotherapy using the Ethos system (Varian Medical Systems, Palo Alto, CA, USA). The first is an 83-year-old male with a remote history of prostate cancer treated with radiotherapy, who received adaptive radiotherapy as a means of decreasing the required margin size and optimizing planning based on adjacent bowel to reduce the risk of re-irradiation. The second patient is a 78-year-old male with node-positive bladder cancer, which necessitated whole pelvis radiotherapy, who underwent adaptive treatment (25 fractions) as a means of sparing cumulative dose to the bowel while ensuring suitable target coverage. In both cases, the clinical target volume consisted of the entire bladder (± nodes) with a planning target volume expansion of 7 mm. During treatment, daily cone-beam CT scans were acquired and used to generate adapted plans. These plans were compared to the original plans, with attention to target coverage and dose to organs at risk. For all 45 fractions, the adaptive plan was selected, primarily as a means of improving target coverage. This case series demonstrates that the adaptive Ethos system effectively delivers treatment for primary bladder cancer. Further data are needed for clinical toxicity outcomes and the efficacy of this approach.
膀胱癌的三联疗法,包括最大程度的经尿道肿瘤切除术,随后进行同步放化疗,是一种具有治愈和保留器官意图的有吸引力的治疗选择。然而,由于膀胱充盈的日常变化需要较大的治疗边界,这种治疗可能会伴有急性毒性反应,从而导致膀胱、肠道和直肠毒性。自适应放疗考虑了膀胱大小的分次间变化,能够以较小的边界将放疗精准地施用于膀胱癌,有可能在不影响靶区覆盖的相关风险的情况下降低毒性。在此,我们展示了一系列两个原发性膀胱癌患者的病例,他们使用Ethos系统(美国瓦里安医疗系统公司,加利福尼亚州帕洛阿尔托)接受了基于计算机断层扫描(CT)的在线自适应低分割放疗。第一个是一名83岁男性,有前列腺癌放疗史,接受自适应放疗以减小所需的边界大小,并根据相邻肠道优化计划,以降低再次放疗的风险。第二个患者是一名78岁男性,患有淋巴结阳性膀胱癌,需要进行全盆腔放疗,他接受了自适应治疗(25次分割),以在确保合适的靶区覆盖的同时减少肠道的累积剂量。在这两个病例中,临床靶区体积包括整个膀胱(±淋巴结),计划靶区体积外放7毫米。在治疗期间,每天获取锥束CT扫描并用于生成自适应计划。将这些计划与原始计划进行比较,关注靶区覆盖和危及器官的剂量。对于所有45次分割,均选择了自适应计划,主要是为了改善靶区覆盖。该病例系列表明,自适应Ethos系统有效地为原发性膀胱癌提供了治疗。还需要进一步的数据来了解临床毒性结果和这种方法的疗效。