Department of Critical Care Medicine, Central Hospital affiliated to Shandong First Medical University, Jinan Central Hospital affiliated to Shandong University, Jinan, China.
Department of Critical Care Medicine, Qilu Hospital of Shandong University, Jinan, China.
Ann Med. 2024 Dec;56(1):2405073. doi: 10.1080/07853890.2024.2405073. Epub 2024 Sep 20.
Thrombocytopenia is commonly observed in patients with sepsis and is an independent risk factor for poor prognosis. However, the changes of platelet count caused by different pathogens can vary significantly. Our study aims to evaluate the quantitative changes in platelet count in response to various pathogens.
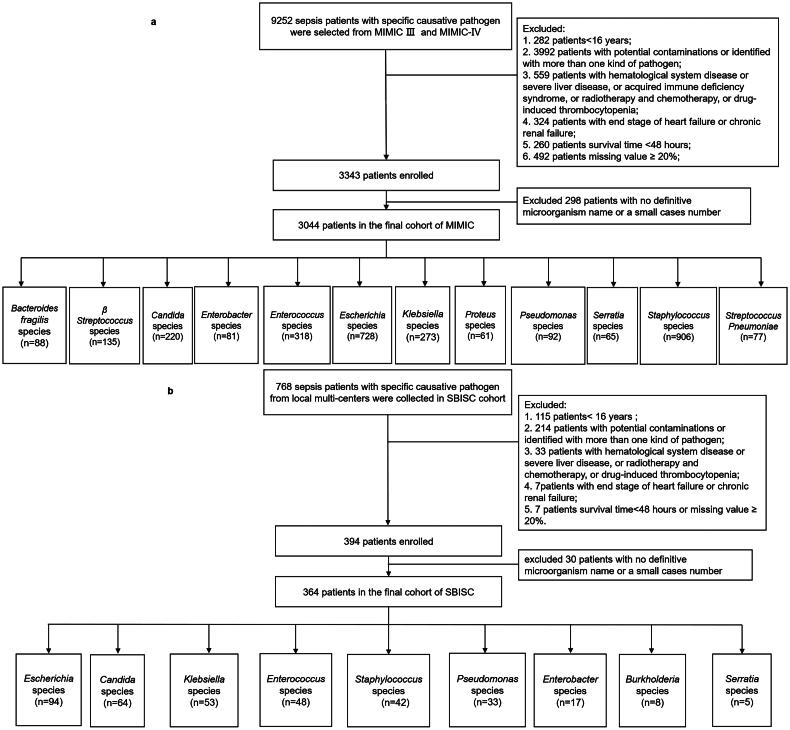
We retrospectively analysed data of 3044 patients with sepsis from Medical Information Mart for Intensive Care (MIMIC, 2008-2019) database and prospectively collected data of 364 patients with sepsis from our local cohort of the Shandong Bloodstream Infection and Sepsis Collaboration Study (SBISC, 2020-2022). Propensity score matching (PSM) was employed to control for baseline differences in variables, except for the causative pathogen.
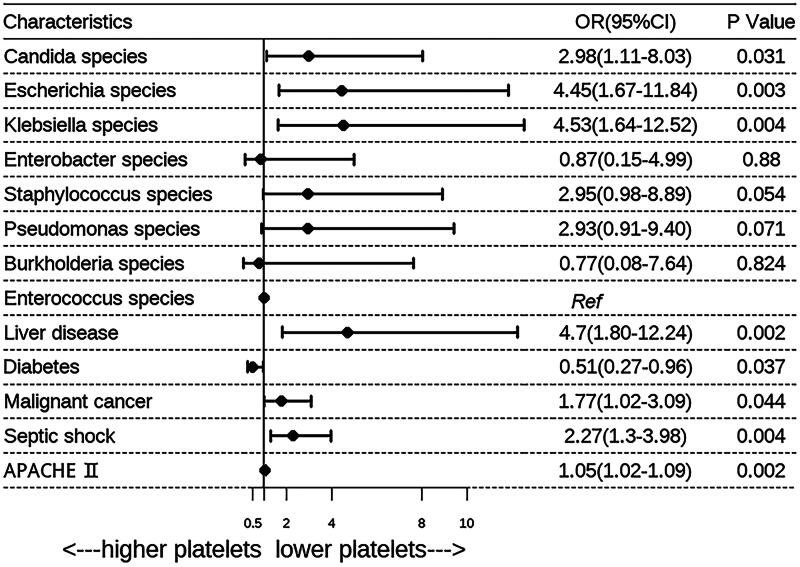
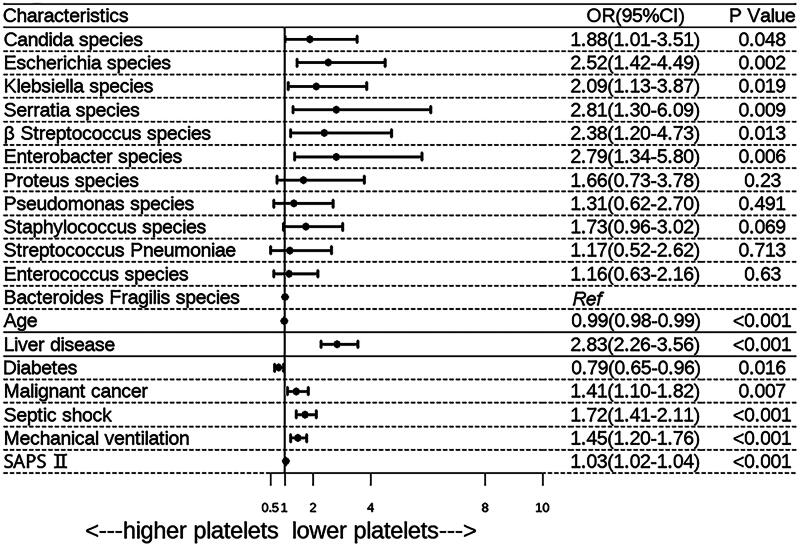
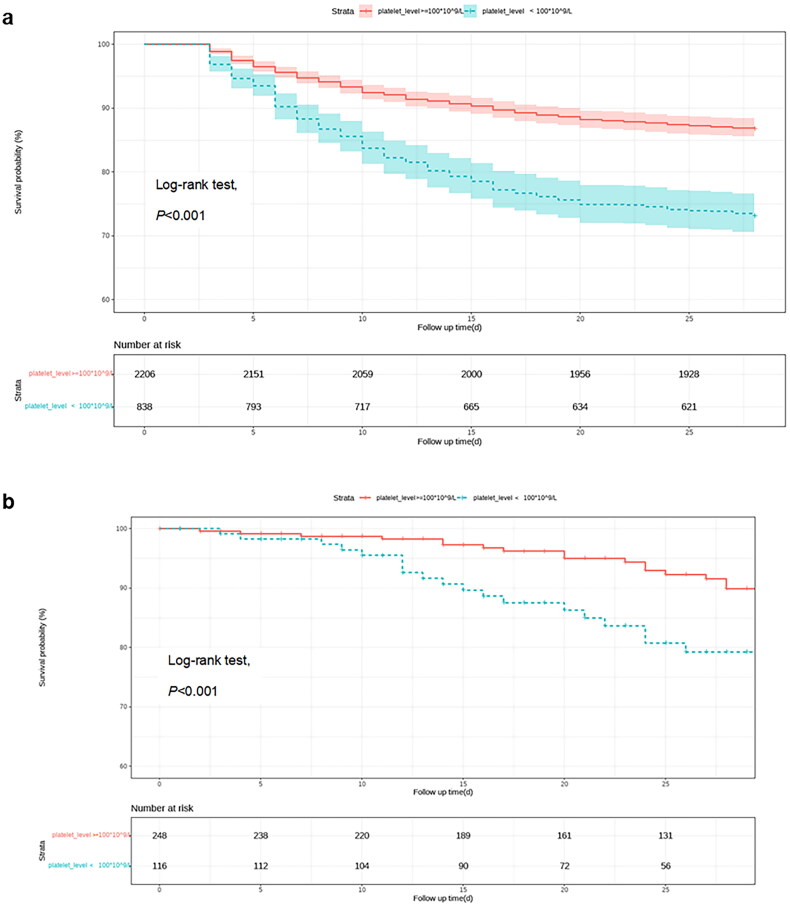
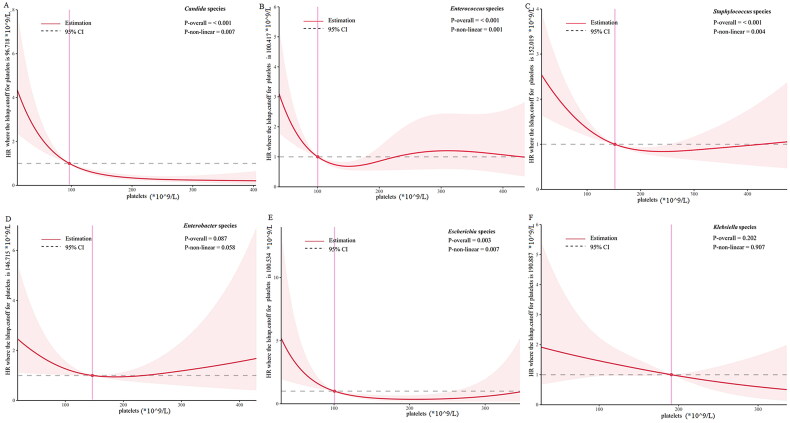
Multivariate logistic analyses of both original and PSM populations identified , , , and species posing a higher risk for thrombocytopenia compared to others. Restricted cubic spline (RCS) curves showed L- or U-shaped associations between platelet count and 28-mortality with various cut-off values among different pathogens: ranging from 96 × 10/L in species - 190 × 10/L in species.
Our present findings indicate a pathogen-specific effect on platelet count, highlighting the importance of monitoring thrombocytopenia in patients infected with above microorganisms. Clinicians need to consider pathogen-specific thresholds when intervene on platelet count.
血小板减少症在脓毒症患者中很常见,是预后不良的独立危险因素。然而,不同病原体引起的血小板计数变化可能有很大差异。我们的研究旨在评估血小板计数对各种病原体的定量变化。
我们回顾性分析了来自医疗信息共享知识库(MIMIC,2008-2019 年)数据库的 3044 例脓毒症患者的数据,并前瞻性收集了来自我们当地山东血流感染和脓毒症合作研究(SBISC,2020-2022 年)队列的 364 例脓毒症患者的数据。除了病原体外,采用倾向评分匹配(PSM)来控制变量的基线差异。
原始和 PSM 人群的多变量逻辑分析表明,与其他病原体相比, 、 、 、 等病原体引起血小板减少症的风险更高。限制性立方样条(RCS)曲线显示,血小板计数与 28 天死亡率之间呈 L 形或 U 形关联,不同病原体的各种截断值范围为 96×10/L( 种)至 190×10/L( 种)。
我们目前的研究结果表明,血小板计数存在病原体特异性效应,强调了监测感染上述微生物的患者血小板减少症的重要性。临床医生在干预血小板计数时需要考虑病原体特异性阈值。