Poli Elizabeth C, Dong Wenli, Shaitelman Simona F, Tamirisa Nina, Shen Yu, Bedrosian Isabelle
Division of Surgical Oncology, Endeavor Health-NorthShore University Health System, Evanston, IL, USA.
Department of Biostatistics, University of Texas, MD Anderson Cancer Center, Houston, TX, USA.
NPJ Breast Cancer. 2024 Sep 20;10(1):82. doi: 10.1038/s41523-024-00689-5.
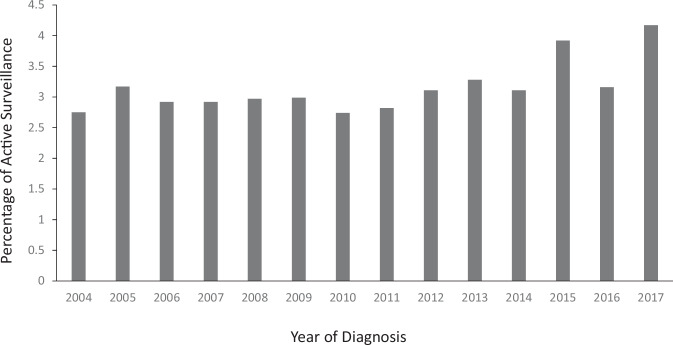
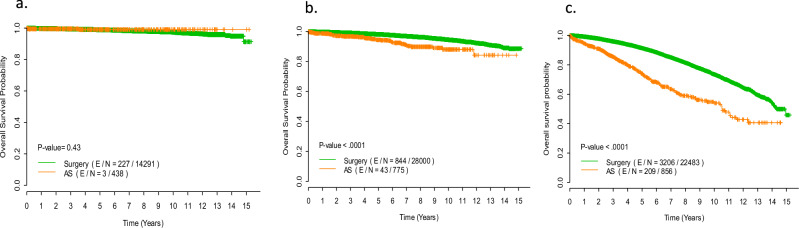
Clinical trials of active surveillance (AS) for Ductal Carcinoma in Situ (DCIS) are underway. We sought to understand the historical management of biologically favorable DCIS and to determine the outcomes of patients who did not have immediate surgery. Using data from the NCDB from 2004 to 2017, the selected cohort included women >40 years of age, with low or intermediate grade and hormone receptor (HR) positive DCIS. AS was defined as either no surgery or surgery >12 months from diagnosis. Women in the AS group were compared to women who had immediate surgery. A Cochran-Armitage test was used to assess the trend of AS over year of diagnosis. Kaplan-Meier curves were estimated to compare overall survival (OS), stratified by age (<50, 50-64, ≥65), and Cox proportional hazard models were used to determine the effects of prognostic factors on survival distributions. 74,367 women met study inclusion criteria; 2384 (3.2%) were treated with AS. The proportion of patients in the AS cohort increased yearly, peaking in 2017 at 4.2% (p < 0.01). On multivariable analysis, increasing age (OR 1.02, p < 0.01), black race (OR 1.7, p < 0.001), and being uninsured (OR 2.2, p < 0.001) were associated with increased likelihood of AS. In women <50 years of age, OS outcomes were similar, with 10-year OS of 97.4% in the immediate surgery cohort versus 99.1% in AS cohort (p = 0.43). The proportion of patients with DCIS treated with AS has remained small but is increasing over time. AS of biologically favorable DCIS in younger, healthier women is not associated with adverse survival.
导管原位癌(DCIS)主动监测(AS)的临床试验正在进行中。我们试图了解生物学上预后良好的DCIS的既往治疗情况,并确定未立即接受手术的患者的预后。利用2004年至2017年国家癌症数据库(NCDB)的数据,选定的队列包括年龄大于40岁、低级别或中级别的激素受体(HR)阳性DCIS女性。AS定义为未进行手术或诊断后12个月以上进行手术。将AS组的女性与立即接受手术的女性进行比较。采用 Cochr an-Armitage检验评估诊断年份中AS的趋势。估计Kaplan-Meier曲线以比较总体生存率(OS),按年龄(<50岁、50 - 64岁、≥65岁)分层,并使用Cox比例风险模型确定预后因素对生存分布的影响。74367名女性符合研究纳入标准;2384名(3.2%)接受了AS治疗。AS队列中的患者比例逐年增加,2017年达到峰值4.2%(p < 0.01)。多变量分析显示,年龄增加(OR 1.02,p < 0.01)、黑人种族(OR 1.7,p < 0.001)和未参保(OR 2.2,p < 0.001)与AS可能性增加相关。在年龄小于50岁的女性中,OS结果相似,立即手术队列的10年OS为97.4%,AS队列中为99.1%(p = 0.43)。接受AS治疗的DCIS患者比例一直较小,但随着时间推移在增加。年轻、健康女性中生物学上预后良好的DCIS进行AS与不良生存无关。