Netea Stejara A, Biesbroek Giske, van Stijn Diana, Nagelkerke Sietse Q, Kuipers Irene M, Kuijpers Taco W
Pediatric Immunology, Rheumatology and Infectious Disease, Emma Children's Hospital, Amsterdam UMC, Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands.
Department of Experimental Immunology, Amsterdam Institute for Infection & Immunity, Amsterdam UMC, University of Amsterdam, 1105 AZ Amsterdam, The Netherlands.
Biomedicines. 2024 Sep 3;12(9):2014. doi: 10.3390/biomedicines12092014.
Kawasaki disease (KD) is a pediatric vasculitis, leading to coronary artery aneurysms (CAAs) in ~4-14%. Attention to the etiology and course of KD was generated by the close mimic of a SARS-CoV-2-induced phenotype, called multisystem inflammatory syndrome in children (MIS-C).
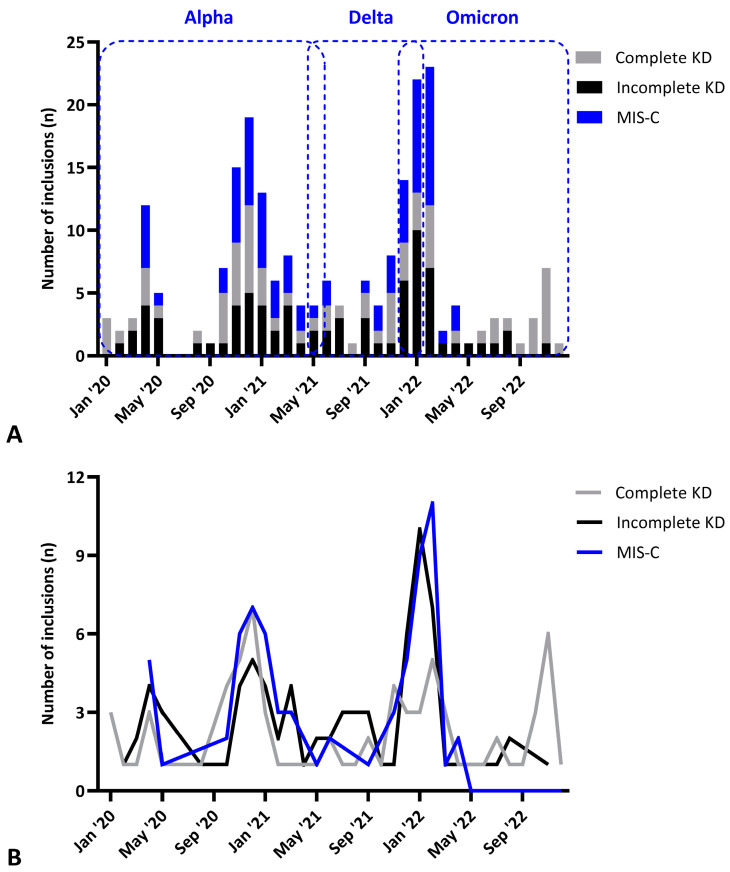
A total of 1179 cases were collected from 2012 with ~50% of cases retrospectively included. Clinical characteristics were described and risk factors for CAA (persistence) were investigated. Phenotypic patterns of the prospectively included KD patients were evaluated. These patterns were also compared to the seronegative KD and seropositive MIS-C cases identified during the SARS-CoV-2 pandemic.
KD mostly affected boys and children < 5 years. IVIG resistance, CAAs, and giant CAAs occurred in 24.5%, 21.4%, and 6.6%, respectively. Giant CAAs were significantly more likely to normalize to a normal score in patients that were younger than 2.5 years old at the time of initial giant CAA (χ test = 0.02). In our prospective (SARS-CoV-2-seronegative) KD series, there was a diminishing male predominance over time, whereas the proportions of incomplete presentations ( < 0.001) and patients with circulatory shock ( = 0.04) increased since the COVID-19 pandemic. Pre- and post-pandemic KD cases presented with different levels of C-reactive protein, thrombocyte counts, and hemoglobin levels over the years. Compared to pandemic KD, SARS-CoV-2-seropositive MIS-C patients were older ( < 0.001), and more often required intensive care admission ( < 0.001), with a gradual decrease over time between 2020 and 2022 ( = 0.04). KD carried a substantial risk of CAA development in contrast to MIS-C.
the phenotypic changes seen over the last twelve years of our prospective follow-up study suggest a spectrum of hyperinflammatory states with potentially different triggering events within this clinical entity.
川崎病(KD)是一种儿科血管炎,约4%-14%的患者会出现冠状动脉瘤(CAA)。儿童多系统炎症综合征(MIS-C)这种由严重急性呼吸综合征冠状病毒2(SARS-CoV-2)诱导的表型与川崎病极为相似,引发了人们对川崎病病因和病程的关注。
收集了2012年以来的1179例病例,约50%的病例为回顾性纳入。描述了临床特征,并调查了CAA(持续性)的危险因素。对前瞻性纳入的川崎病患者的表型模式进行了评估。还将这些模式与在SARS-CoV-2大流行期间确定的血清阴性川崎病和血清阳性MIS-C病例进行了比较。
川崎病主要影响男孩和5岁以下儿童。静脉注射免疫球蛋白(IVIG)抵抗、CAA和巨大CAA的发生率分别为24.5%、21.4%和6.6%。在初次出现巨大CAA时年龄小于2.5岁的患者中,巨大CAA更有可能恢复到正常评分(χ检验=0.02)。在我们的前瞻性(SARS-CoV-2血清阴性)川崎病系列中,随着时间的推移,男性优势逐渐减弱,而自2019冠状病毒病大流行以来,不完全表现(<0.001)和循环休克患者的比例(=0.04)有所增加。多年来,大流行前和大流行后的川崎病病例呈现出不同水平的C反应蛋白、血小板计数和血红蛋白水平。与大流行期间的川崎病相比,SARS-CoV-2血清阳性MIS-C患者年龄更大(<0.001),更常需要入住重症监护病房(<0.001),在2020年至2022年期间随时间逐渐减少(=0.04)。与MIS-C相比,川崎病发生CAA的风险很大。
在我们为期十二年的前瞻性随访研究中观察到的表型变化表明,在这个临床实体中存在一系列具有潜在不同触发事件的过度炎症状态。