Department of Cardiology, "Carol Davila" University of Medicine and Pharmacy, "Prof. Dr. Theodor Burghele" Clinical Hospital, 010024 Bucharest, Romania.
Dr. Carol Davila University Central Military Emergency Hospital, 010825 Bucharest, Romania.
Medicina (Kaunas). 2024 Sep 6;60(9):1466. doi: 10.3390/medicina60091466.
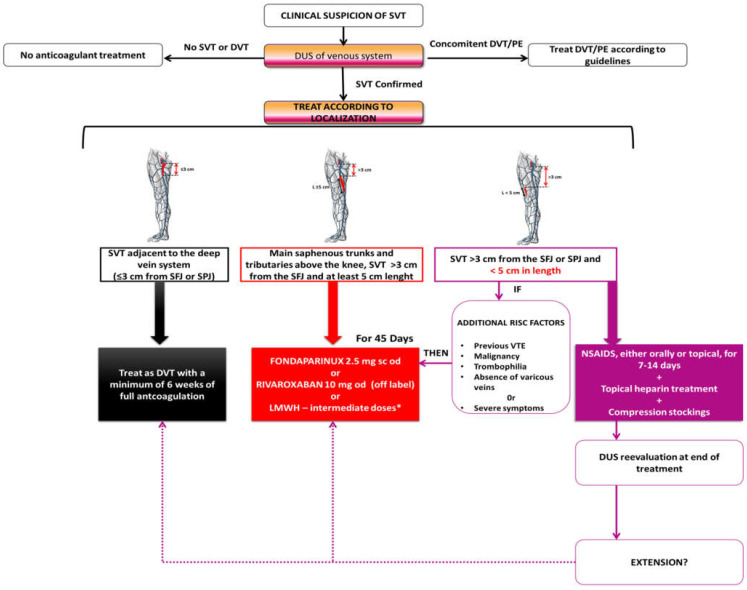
Superficial venous thrombosis (SVT) is a fairly common disorder, characterized by the formation of thrombi inside superficial veins, with or without an associated inflammatory reaction. Its evolution is frequently self-limited. However, serious complications may change this clinical course with extension to deep vein thrombosis (DVT) and pulmonary embolism (PE). SVT shares similar risk factors with DVT and is frequently associated with the presence of varicose veins. However, the occurrence of non-varicose veins could conceal risk factors such as malignancies, thrombophilia, or Buerger's disease. While the clinical diagnosis is generally straightforward, additional diagnostic evaluations are often necessary. Duplex ultrasound (DUS) is an invaluable tool that provides the location of SVT, the proximity to the sapheno-femoral junction, and the clot length, all of which influence the decision for optimal management. The treatment of SVT should be symptomatic, pathogenic (limiting the extension of thrombosis), and prognostic (to prevent complications). There are several guidelines that provide recommendations, and despite the need for more consensus and for further studies, the treatment of SVT should be mainly medical, including anticoagulation in specific clinical situations and symptom relief, with invasive treatment in a minority of cases. Initiation, intensity, and length of anticoagulant treatment should be based on the eventual risk of progression to DVT or PE, which can be high, intermediate, or low, based on the location of SVT and the clot length. Our review summarizes the evaluation and proper management of SVT and highlights the importance of a shared decision within the heart team regarding this condition in order to prevent further complications.
浅静脉血栓形成(SVT)是一种相当常见的疾病,其特征是浅静脉内血栓形成,伴有或不伴有炎症反应。其演变通常是自限性的。然而,严重的并发症可能会改变这种临床过程,导致深静脉血栓形成(DVT)和肺栓塞(PE)。SVT 与 DVT 有相似的危险因素,常与静脉曲张有关。然而,非静脉曲张的发生可能隐藏了恶性肿瘤、血栓形成倾向或伯格氏病等危险因素。虽然临床诊断通常很简单,但通常需要额外的诊断评估。双功能超声(DUS)是一种非常有价值的工具,它可以提供 SVT 的位置、靠近股隐静脉交界处的位置以及血栓的长度,所有这些都影响最佳管理决策。SVT 的治疗应是对症、针对病因(限制血栓延伸)和预测预后(预防并发症)的。有几个指南提供了建议,尽管需要更多的共识和进一步的研究,但 SVT 的治疗主要应该是药物治疗,包括在特定临床情况下抗凝和缓解症状,少数情况下需要侵入性治疗。抗凝治疗的开始、强度和持续时间应基于向 DVT 或 PE 进展的最终风险,这可以根据 SVT 的位置和血栓长度分为高、中、低风险。我们的综述总结了 SVT 的评估和适当管理,并强调了在心脏团队内就这种情况做出共同决策的重要性,以预防进一步的并发症。