Biophysics, Center for Integrative Physiology and Molecular Medicine (CIPMM), School of Medicine, Saarland University, Building 48, 66421, Homburg, Germany.
Department of Medical Biometry, Epidemiology and Medical Informatics, Saarland University, Medical Center, 66421, Homburg, Germany.
Mol Cancer. 2024 Sep 28;23(1):210. doi: 10.1186/s12943-024-02123-7.
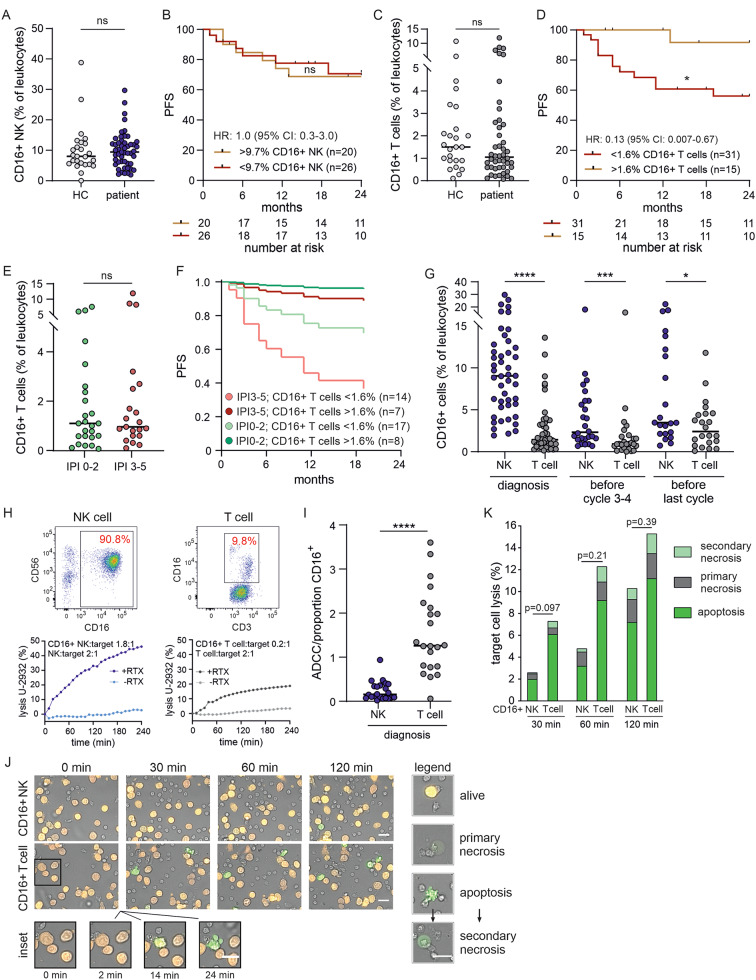
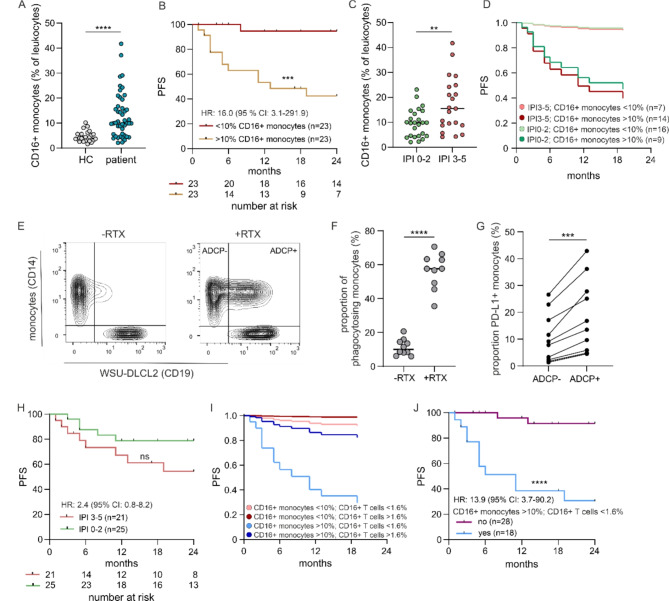
Assessing the prognosis of patients with aggressive non-Hodgkin B cell lymphoma mainly relies on a clinical risk score (IPI). Standard first-line therapies are based on a chemo-immunotherapy with rituximab, which mediates CD16-dependent antibody-dependent cellular cytotoxicity (ADCC). We phenotypically and functionally analyzed blood samples from 46 patients focusing on CD16+ NK cells, CD16+ T cells and CD16+ monocytes. Kaplan-Meier survival curves show a superior progression-free survival (PFS) for patients having more than 1.6% CD16+ T cells (p = 0.02; HR = 0.13 (0.007-0.67)) but an inferior PFS having more than 10.0% CD16+ monocytes (p = 0.0003; HR = 16.0 (3.1-291.9)) at diagnosis. Surprisingly, no correlation with NK cells was found. The increased risk of relapse in the presence of > 10.0% CD16+ monocytes is reversed by the simultaneous occurrence of > 1.6% CD16+ T cells. The unexpectedly strong protective function of CD16+ T cells could be explained by their high antibody-dependent cellular cytotoxicity as quantified by real-time killing assays and single-cell imaging. The combined analysis of CD16+ monocytes (> 10%) and CD16+ T cells (< 1.6%) provided a strong model with a Harrell's C index of 0.80 and a very strong power of 0.996 even with our sample size of 46 patients. CD16 assessment in the initial blood analysis is thus a precise marker for early relapse prediction.
评估侵袭性非霍奇金 B 细胞淋巴瘤患者的预后主要依赖于临床风险评分(IPI)。标准一线治疗基于含利妥昔单抗的化疗-免疫治疗,该治疗通过 CD16 依赖性抗体依赖性细胞细胞毒性(ADCC)发挥作用。我们对 46 例患者的血液样本进行了表型和功能分析,重点关注 CD16+NK 细胞、CD16+T 细胞和 CD16+单核细胞。Kaplan-Meier 生存曲线显示,具有超过 1.6%CD16+T 细胞的患者无进展生存期(PFS)更好(p=0.02;HR=0.13(0.007-0.67)),而具有超过 10.0%CD16+单核细胞的患者 PFS 更差(p=0.0003;HR=16.0(3.1-291.9))。令人惊讶的是,未发现与 NK 细胞相关。在诊断时存在 >10.0%CD16+单核细胞的情况下,复发风险增加,但同时存在 >1.6%CD16+T 细胞时,这种风险会降低。CD16+T 细胞具有出乎意料的强大保护作用,这可以通过实时杀伤测定和单细胞成像定量的其高抗体依赖性细胞毒性来解释。CD16+单核细胞(>10%)和 CD16+T 细胞(<1.6%)的联合分析提供了一个强大的模型,哈雷尔 C 指数为 0.80,即使在我们的 46 例患者样本中,其效能也非常强,为 0.996。因此,初始血液分析中的 CD16 评估是早期复发预测的精确标志物。