Yoon Soo-Hyuk, Choi Seungeun, Yoon Susie, Na Kwon Joong, Bahk Jaehyon, Lee Ho-Jin
Department of Anesthesiology and Pain Medicine, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
Department of Thoracic and Cardiovascular Surgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
Korean J Pain. 2024 Oct 1;37(4):354-366. doi: 10.3344/kjp.24173.
Anesthetic agents are potential modifiable factors that can mitigate chronic postsurgical pain (CPSP) development. This study aimed to investigate the association between propofol-based total intravenous anesthesia (TIVA) and the occurrence of CPSP following video-assisted thoracoscopic surgery (VATS) for lung cancer resection.
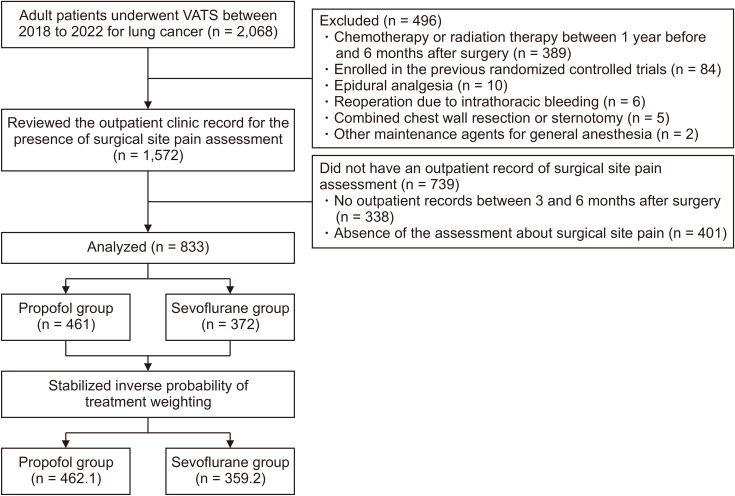
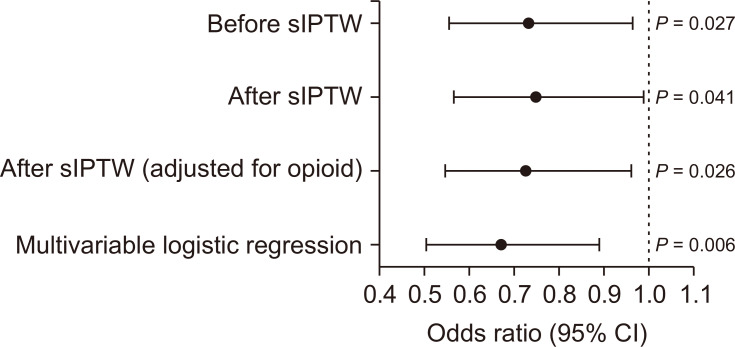
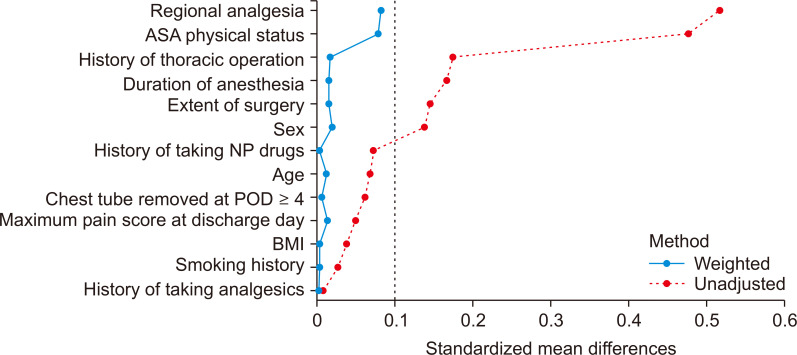
This single-center retrospective cohort study included adult patients with lung cancer who underwent elective VATS between January 2018 and December 2022. Patients were divided based on the maintenance anesthetic used (propofol vs. sevoflurane). The primary outcome was the presence of CPSP, defined as any level of surgical site pain recorded within 3-6 months postoperatively. The authors investigated the association between anesthetic agents and CPSP using propensity score matching with stabilized inverse probability of treatment weighting (sIPTW) to adjust for confounders. Additionally, multivariable logistic regression was used to further adjust for intraoperative opioid use that sIPTW could not account for. The robustness of these associations was evaluated using the E-value.
Of the 833 patients analyzed, 461 received propofol and 372 sevoflurane. The overall incidence of CPSP was 43.3%. After sIPTW, the use of TIVA was significantly associated with a lower incidence of CPSP (odds ratio [OR]: 0.75, 95% confidence interval [CI]: 0.57-0.99, = 0.041), and remained significant after adjusting for intraoperative remifentanil equivalent dose (OR: 0.73, 95% CI: 0.55-0.96, = 0.026). The E-values were 1.08 and 1.17, respectively.
Propofol-based TIVA is associated with reduced CPSP occurrence in VATS for lung cancer. Further prospective studies are needed to confirm the results.
麻醉药物是可减轻慢性术后疼痛(CPSP)发生的潜在可调节因素。本研究旨在探讨基于丙泊酚的全静脉麻醉(TIVA)与肺癌切除电视辅助胸腔镜手术(VATS)后CPSP发生之间的关联。
这项单中心回顾性队列研究纳入了2018年1月至2022年12月期间接受择期VATS的成年肺癌患者。根据维持麻醉用药(丙泊酚与七氟醚)对患者进行分组。主要结局是CPSP的存在,定义为术后3至6个月内记录的任何程度的手术部位疼痛。作者使用倾向评分匹配和稳定化治疗权重逆概率(sIPTW)来调整混杂因素,研究麻醉药物与CPSP之间的关联。此外,使用多变量逻辑回归进一步调整sIPTW无法解释的术中阿片类药物使用情况。使用E值评估这些关联的稳健性。
在分析的833例患者中,461例接受丙泊酚,372例接受七氟醚。CPSP的总体发生率为43.3%。经过sIPTW后,TIVA的使用与较低的CPSP发生率显著相关(比值比[OR]:0.75,95%置信区间[CI]:0.57 - 0.99,P = 0.041),在调整术中瑞芬太尼等效剂量后仍具有显著性(OR:0.73,95% CI:0.55 - 0.96,P = 0.026)。E值分别为1.08和1.17。
基于丙泊酚的TIVA与VATS肺癌手术中CPSP发生率降低相关。需要进一步的前瞻性研究来证实这些结果。