Salié Henrike, Wischer Lara, D'Alessio Antonio, Godbole Ira, Suo Yuan, Otto-Mora Patricia, Beck Juergen, Neumann Olaf, Stenzinger Albrecht, Schirmacher Peter, Fulgenzi Claudia A M, Blaumeiser Andreas, Boerries Melanie, Roehlen Natascha, Schultheiß Michael, Hofmann Maike, Thimme Robert, Pinato David J, Longerich Thomas, Bengsch Bertram
Department of Internal Medicine II, Medical Center - University of Freiburg, Freiburg, Germany.
Department of Surgery & Cancer, Imperial College London, London, UK.
Gut. 2025 Feb 6;74(3):451-466. doi: 10.1136/gutjnl-2024-332837.
The determinants of the response to checkpoint immunotherapy in hepatocellular carcinoma (HCC) remain poorly understood. The organisation of the immune response in the tumour microenvironment (TME) is expected to govern immunotherapy outcomes but spatial immunotypes remain poorly defined.
We hypothesised that the deconvolution of spatial immune network architectures could identify clinically relevant immunotypes in HCC.
We conducted highly multiplexed imaging mass cytometry on HCC tissues from 101 patients. We performed in-depth spatial single-cell analysis in a discovery and validation cohort to deconvolute the determinants of the heterogeneity of HCC immune architecture and develop a spatial immune classification that was tested for the prediction of immune checkpoint inhibitor (ICI) therapy.
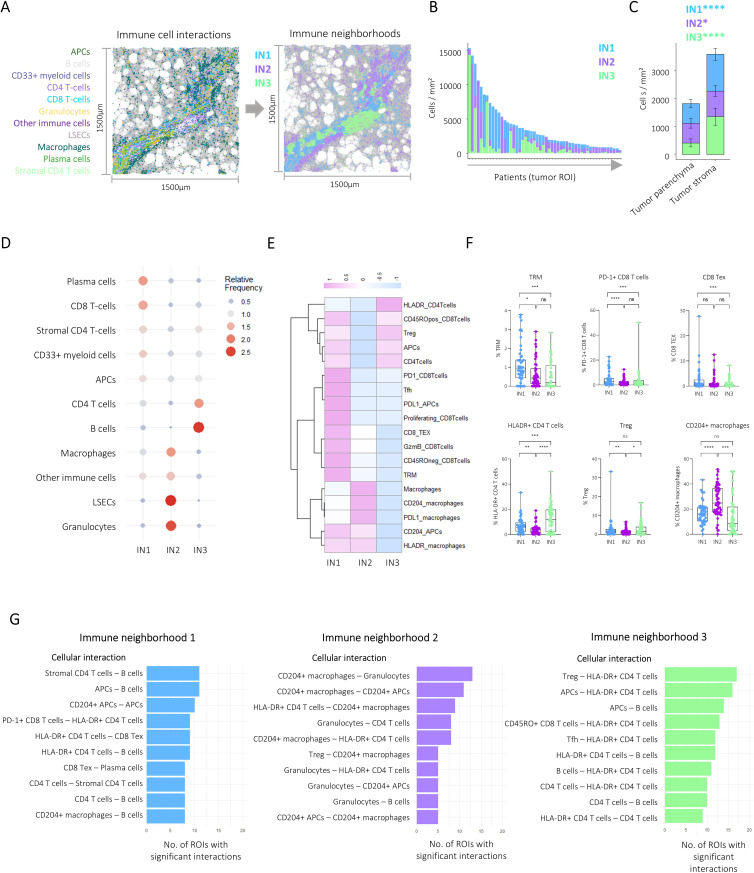
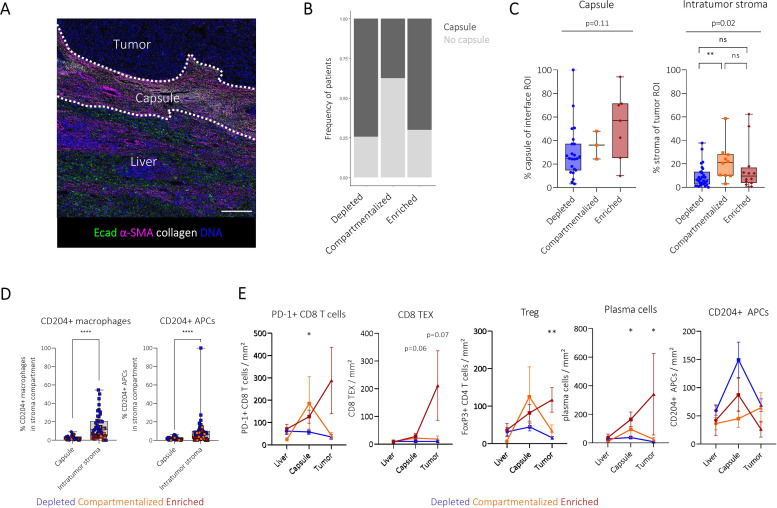
Bioinformatic analysis identified 23 major immune, stroma, parenchymal and tumour cell types in the HCC TME. Unsupervised neighbourhood detection based on the spatial interaction of immune cells identified three immune architectures with differing involvement of immune cells and immune checkpoints dominated by either CD8 T-cells, myeloid immune cells or B- and CD4 T-cells. We used these to define three major spatial HCC immunotypes that reflect a higher level of intratumour immune cell organisation: depleted, compartmentalised and enriched. Progression-free survival under ICI therapy differed significantly between the spatial immune types with improved survival of enriched patients. In patients with intratumour heterogeneity, the presence of one enriched area governed long-term survival.
肝细胞癌(HCC)中对免疫检查点免疫疗法反应的决定因素仍知之甚少。肿瘤微环境(TME)中的免疫反应组织有望决定免疫治疗结果,但空间免疫类型仍定义不清。
我们假设空间免疫网络架构的反卷积可以识别HCC中临床相关的免疫类型。
我们对101例患者的HCC组织进行了高度多重成像质谱流式细胞术分析。我们在一个发现队列和验证队列中进行了深入的空间单细胞分析,以反卷积HCC免疫结构异质性的决定因素,并开发一种空间免疫分类方法,用于测试免疫检查点抑制剂(ICI)治疗的预测效果。
生物信息学分析在HCC的TME中鉴定出23种主要的免疫、基质、实质和肿瘤细胞类型。基于免疫细胞的空间相互作用进行的无监督邻域检测识别出三种免疫结构,其免疫细胞和免疫检查点的参与程度不同,分别以CD8 T细胞、髓系免疫细胞或B细胞和CD4 T细胞为主。我们用这些来定义三种主要的空间HCC免疫类型,它们反映了肿瘤内免疫细胞组织的更高水平:耗竭型(depleted)、分隔型(compartmentalised)和富集型(enriched)。ICI治疗下的无进展生存期在不同空间免疫类型之间有显著差异,富集型患者的生存期有所改善。在肿瘤内存在异质性的患者中,一个富集区域的存在决定了长期生存。