Clinical Cooperation Unit Molecular Hematology/Oncology, German Cancer Research Center (DKFZ) and Department of Internal Medicine V, University of Heidelberg, Heidelberg, Germany.
Department of Internal Medicine V, University of Heidelberg, Heidelberg, Germany.
Nat Commun. 2023 Oct 24;14(1):6761. doi: 10.1038/s41467-023-42400-5.
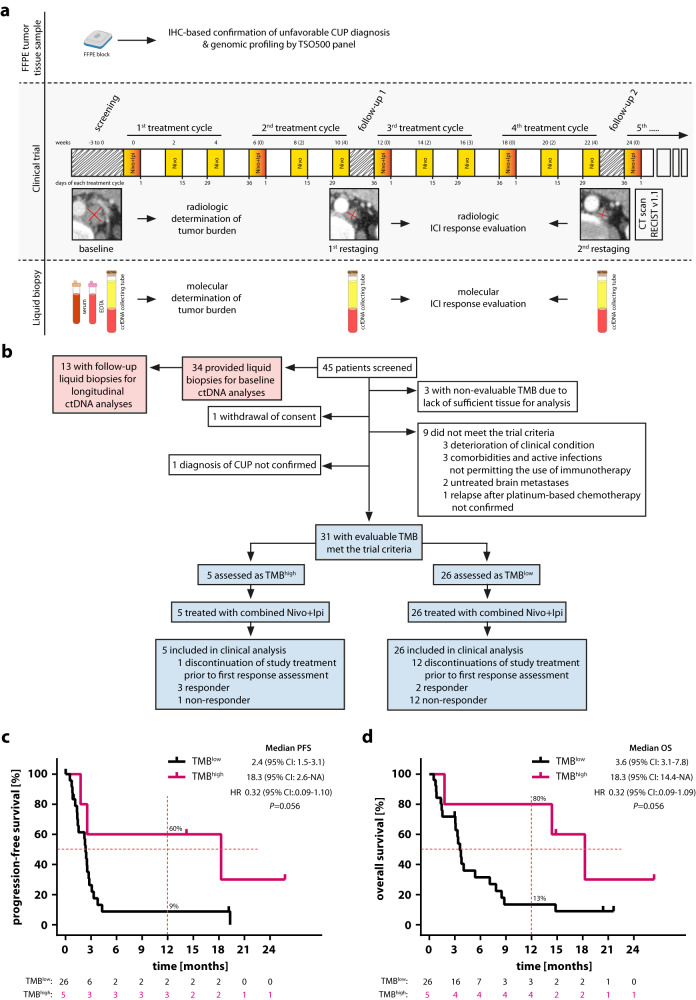
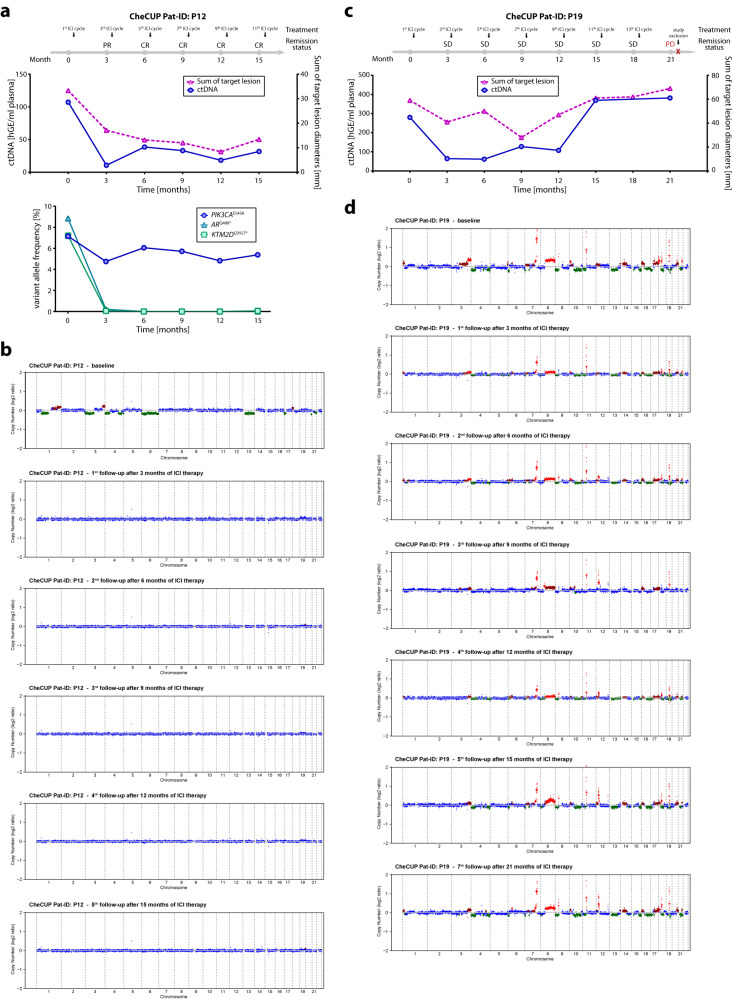
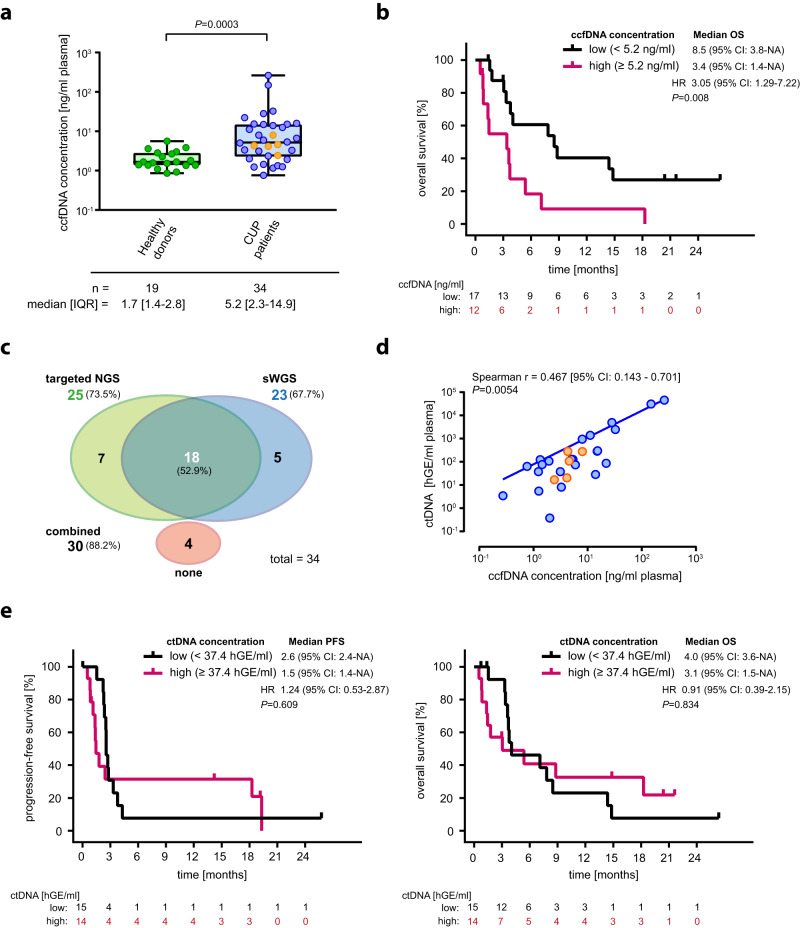
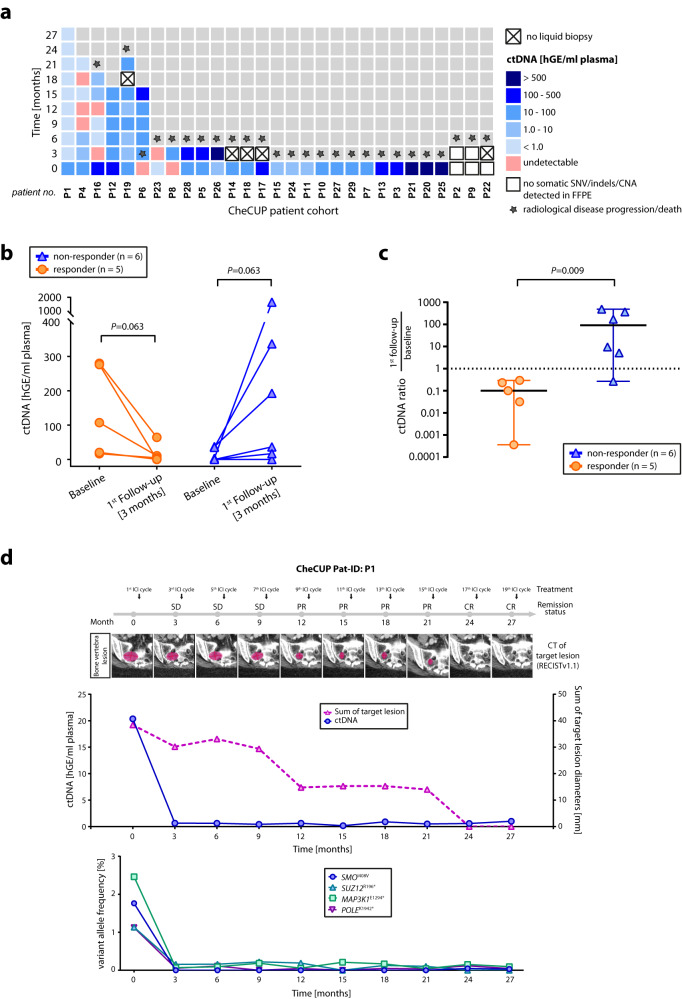
Cancer of unknown primary has a dismal prognosis, especially following failure of platinum-based chemotherapy. 10-20% of patients have a high tumor mutational burden (TMB), which predicts response to immunotherapy in many cancer types. In this prospective, non-randomized, open-label, multicenter Phase II trial (EudraCT 2018-004562-33; NCT04131621), patients relapsed or refractory after platinum-based chemotherapy received nivolumab and ipilimumab following TMB vs. TMB stratification. Progression-free survival (PFS) represented the primary endpoint; overall survival (OS), response rates, duration of clinical benefit and safety were the secondary endpoints. The trial was prematurely terminated in March 2021 before reaching the preplanned sample size (n = 194). Among 31 evaluable patients, 16% had a high TMB ( > 12 mutations/Mb). Overall response rate was 16% (95% CI 6-34%), with 7.7% (95% CI 1-25%) vs. 60% (95% CI 15-95%) in TMB and TMB, respectively. Although the primary endpoint was not met, high TMB was associated with better median PFS (18.3 vs. 2.4 months) and OS (18.3 vs. 3.6 months). Severe immune-related adverse events were reported in 29% of cases. Assessing on-treatment dynamics of circulating tumor DNA using combined targeted hotspot mutation and shallow whole genome sequencing as part of a predefined exploratory analysis identified patients benefiting from immunotherapy irrespective of initial radiologic response.
原发灶不明癌预后较差,尤其是在铂类化疗失败后。10-20%的患者存在高肿瘤突变负荷(TMB),这预示着许多癌症类型对免疫治疗有反应。在这项前瞻性、非随机、开放标签、多中心 II 期试验(EudraCT 2018-004562-33;NCT04131621)中,铂类化疗后复发或耐药的患者根据 TMB 与 TMB 分层接受纳武利尤单抗和伊匹单抗治疗。无进展生存期(PFS)是主要终点;总生存期(OS)、缓解率、临床获益持续时间和安全性是次要终点。在达到预定样本量(n=194)之前,该试验于 2021 年 3 月提前终止。在 31 名可评估患者中,16%的患者 TMB 较高(>12 个突变/Mb)。总缓解率为 16%(95%CI 6-34%),TMB 高和 TMB 低的缓解率分别为 7.7%(95%CI 1-25%)和 60%(95%CI 15-95%)。虽然主要终点未达到,但 TMB 较高与更好的中位 PFS(18.3 与 2.4 个月)和 OS(18.3 与 3.6 个月)相关。29%的病例报告了严重的免疫相关不良事件。作为预先定义的探索性分析的一部分,使用联合靶向热点突变和浅层全基因组测序评估循环肿瘤 DNA 的治疗中动态,可识别出无论初始影像学反应如何均受益于免疫治疗的患者。