Verreck Eline E F, Kuijer Anne, van Steenhoven Julia E C, Volders José H, van der Velden Annette W G, Siesling Sabine, Timmer-Bonte Anja N H, Smilde Tineke J, Imholz Alex L T, Blanken-Peeters Charlotte F J M, de Valk Bart, Vrijaldenhoven Suzan, Lastdrager Willem B, Haringhuizen Annebeth W, Hunting Jarmo C B, Hovenga Sjoerd, Nieboer Peter, Zuetenhorst Hanneke M, Tetteroo Geert W M, Smorenburg Carolien H, van Maaren Marissa C, van Dalen Thijs
University Utrecht, Utrecht, the Netherlands.
Department of Surgery, Diakonessenhuis, Bosboomstraat 1, 3582 KE, Utrecht, the Netherlands.
Breast Cancer Res Treat. 2025 Jan;209(2):331-340. doi: 10.1007/s10549-024-07496-3. Epub 2024 Sep 30.
A previous prospective multicenter study revealed the change of the oncologists' chemotherapy advice due to the 70-Gene signature (GS) test result in half of the estrogen receptor-positive (ER+) invasive early-stage breast cancer patients with disputable chemotherapy indication. This resulted in less patients receiving chemotherapy. This study aims to complement these results by the 7-year oncological outcomes according to the 70-GS test result and the oncologists' pre-test advice.
Patients operated for early-stage ER+ breast cancer with disputable chemotherapy indication, had been prospectively included between 2013 and 2015. Oncologists were asked whether they intended to administer adjuvant chemotherapy before deployment of the 70-GS test. Information on adjuvant systemic treatment and oncological outcome was obtained through active follow-up by data managers of the Netherlands Cancer Registry. The primary endpoint of this study was distant metastasis-free survival (DMFS) according to the genomic risk. Exploratory analyses were done to evaluate DMFS in relation to the oncologists' pre-test advice.
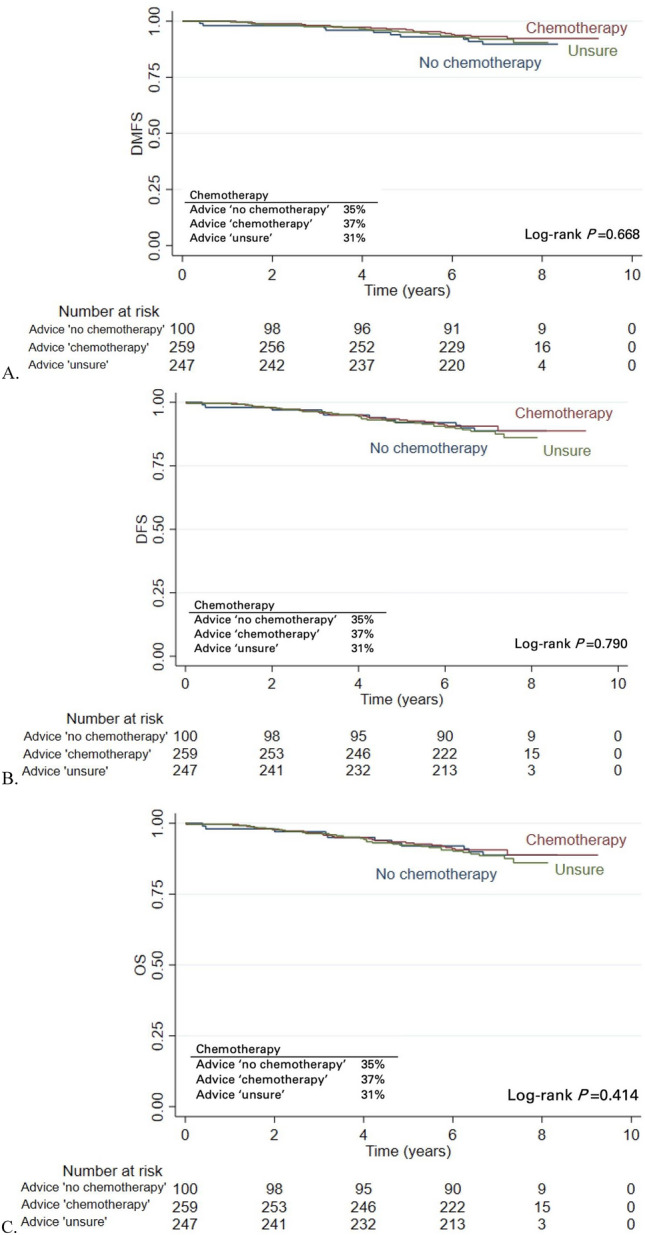
After a median follow-up of 7 years, distant metastases were diagnosed in 23 of the 606 patients (3.8%) and 36 (5.9%) patients had died. The DMFS rate for the 357 70-GS genomic low-risk patients was 94.2% (95% CI 91.2-96.2) and 89.1% for the 249 genomic high-risk patients (95% CI 84.3-92.4). Of the low-risk patients 3% had received chemotherapy compared to 80% of the high-risk patients. For the subgroups based on the pre-test oncologists' advice (no chemotherapy/chemotherapy/unsure) there were no clinically relevant differences in DMFS (89.8, 93.2 and 92.0%, respectively), while comparable proportions of patients had received chemotherapy.
In patients with early-stage ER+ breast cancer with a disputable chemotherapy indication it is sensible to deploy the 70-GS to better select patients for adjuvant chemotherapy.
先前一项前瞻性多中心研究显示,在半数化疗指征存在争议的雌激素受体阳性(ER+)早期浸润性乳腺癌患者中,70基因检测(GS)结果改变了肿瘤学家的化疗建议。这导致接受化疗的患者减少。本研究旨在根据70-GS检测结果和肿瘤学家的检测前建议,通过7年的肿瘤学结局来补充这些结果。
2013年至2015年期间前瞻性纳入了因早期ER+乳腺癌接受手术且化疗指征存在争议的患者。在进行70-GS检测之前,询问肿瘤学家是否打算给予辅助化疗。通过荷兰癌症登记处的数据管理人员进行主动随访,获取辅助全身治疗和肿瘤学结局的信息。本研究的主要终点是根据基因组风险的无远处转移生存期(DMFS)。进行探索性分析以评估与肿瘤学家检测前建议相关的DMFS。
中位随访7年后,606例患者中有23例(3.8%)被诊断为远处转移,36例(5.9%)患者死亡。357例70-GS基因组低风险患者的DMFS率为94.2%(95%CI 91.2-96.2),249例基因组高风险患者的DMFS率为89.1%(95%CI 84.3-92.4)。低风险患者中3%接受了化疗,而高风险患者中这一比例为80%。对于基于检测前肿瘤学家建议(不化疗/化疗/不确定)的亚组,DMFS无临床相关差异(分别为89.8%、93.2%和92.0%),而接受化疗的患者比例相当。
对于化疗指征存在争议的早期ER+乳腺癌患者,应用70-GS来更好地选择辅助化疗患者是合理的。