Choi Ariel R, D'Agostino Ralph B, Farris Michael K, Abdulhaleem Mohammed, Hunting John C, Wang Yuezhu, Smith Margaret R, Ruiz Jimmy, Lycan Thomas W, Petty W Jeffrey, Cramer Christina K, Tatter Stephen B, Laxton Adrian W, White Jaclyn J, Li Wencheng, Su Jing, Whitlow Christopher, Xing Fei, Chan Michael D
Department of Radiation Oncology, Wake Forest School of Medicine, Winston-Salem, NC, United States.
Department of Biostatistics and Data Science, Wake Forest School of Medicine, Winston-Salem, NC, United States.
Front Endocrinol (Lausanne). 2024 Sep 17;15:1364021. doi: 10.3389/fendo.2024.1364021. eCollection 2024.
PURPOSE/OBJECTIVES: Biomarkers for extracranial oligometastatic disease remain elusive and few studies have attempted to correlate genomic data to the presence of true oligometastatic disease.
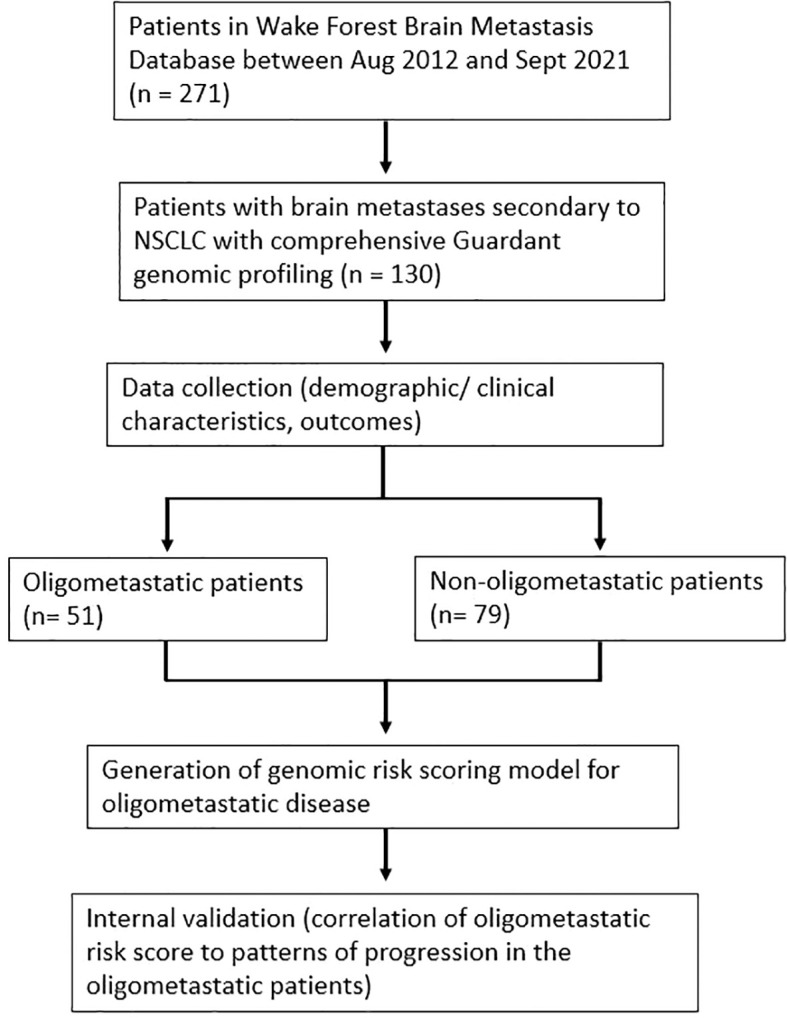
Patients with non-small cell lung cancer (NSCLC) and brain metastases were identified in our departmental database. Electronic medical records were used to identify patients for whom liquid biopsy-based comprehensive genomic profiling (Guardant Health) was available. Extracranial oligometastatic disease was defined as patients having ≤5 non-brain metastases without diffuse involvement of a single organ. Widespread disease was any spread beyond oligometastatic. Fisher's exact tests were used to screen for mutations statistically associated (p<0.1) with either oligometastatic or widespread extracranial disease. A risk score for the likelihood of oligometastatic disease was generated and correlated to the likelihood of having oligometastatic disease vs widespread disease. For oligometastatic patients, a competing risk analysis was done to assess for cumulative incidence of oligometastatic progression. Cox regression was used to determine association between oligometastatic risk score and oligoprogression.
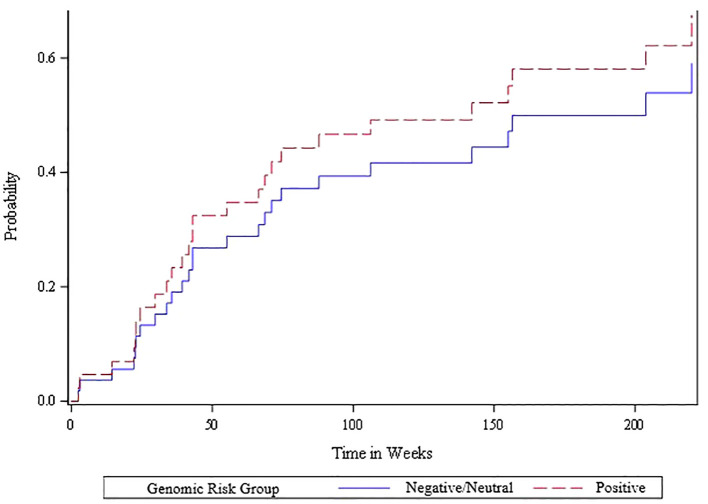
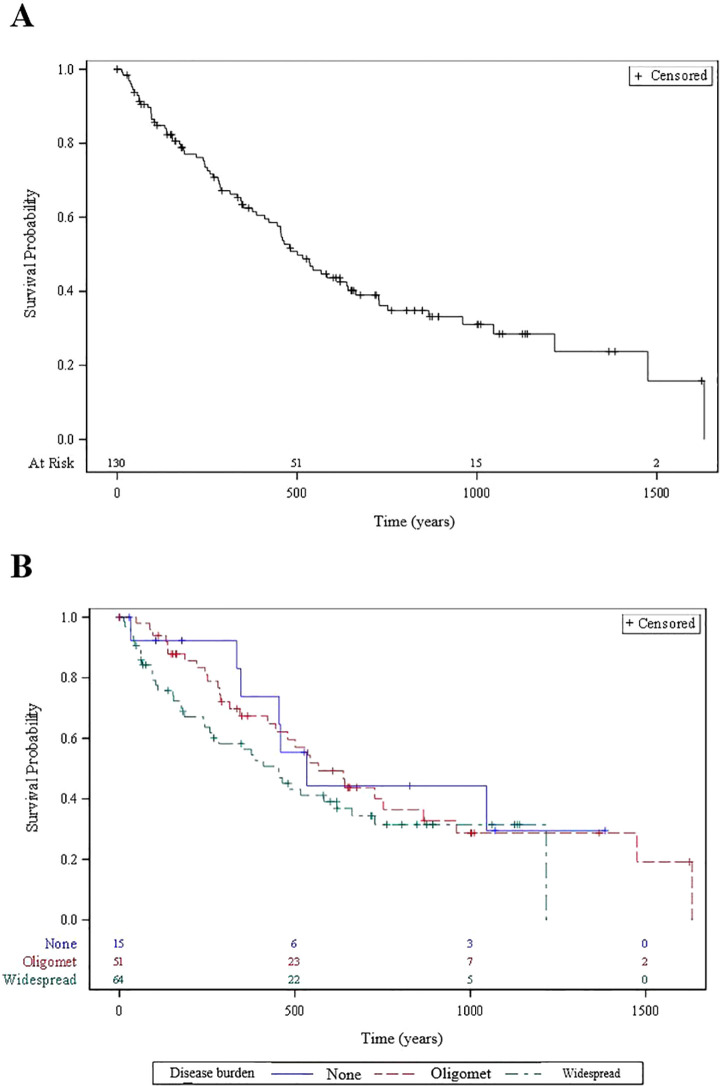
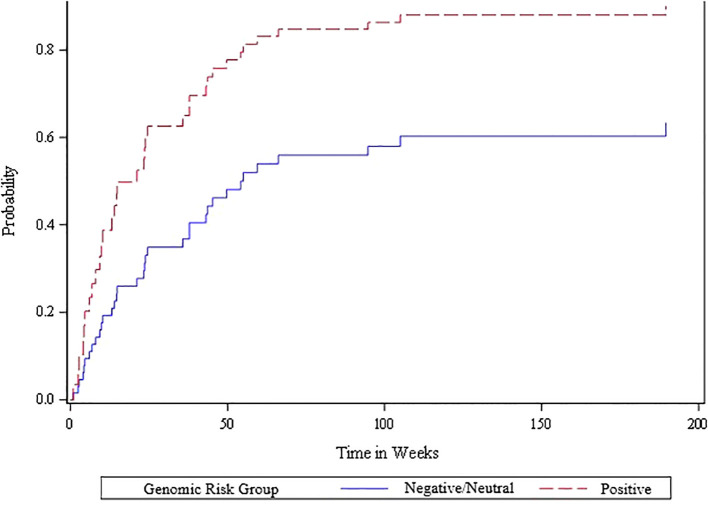
130 patients met study criteria and were included in the analysis. 51 patients (39%) had extracranial oligometastatic disease. Genetic mutations included in the Guardant panel that were associated (p<0.1) with the presence of oligometastatic disease included ATM, JAK2, MAP2K2, and NTRK1, while ARID1A and CCNE1 were associated with widespread disease. Patients with a positive, neutral and negative risk score for oligometastatic disease had a 78%, 41% and 11.5% likelihood of having oligometastatic disease, respectively (p<0.0001). Overall survival for patients with positive, neutral and negative risk scores for oligometastatic disease was 86% vs 82% vs 64% at 6 months (p=0.2). Oligometastatic risk score was significantly associated with the likelihood of oligoprogression based on the Wald chi-square test. Patients with positive, neutral and negative risk scores for oligometastatic disease had a cumulative incidence of oligometastatic progression of 77% vs 35% vs 33% at 6 months (p=0.03).
Elucidation of a genomic signature for extracranial oligometastatic disease derived from non-invasive liquid biopsy appears feasible for NSCLC patients. Patients with this signature exhibited higher rates of early oligoprogression. External validation could lead to a biomarker that has the potential to direct local therapies in oligometastatic patients.
目的/目标:用于颅外寡转移疾病的生物标志物仍然难以捉摸,很少有研究尝试将基因组数据与真正的寡转移疾病的存在相关联。
在我们科室的数据库中识别出患有非小细胞肺癌(NSCLC)和脑转移的患者。使用电子病历识别可获得基于液体活检的综合基因组分析(Guardant Health)的患者。颅外寡转移疾病定义为非脑转移灶≤5个且单个器官无弥漫性受累的患者。广泛转移疾病是指超出寡转移范围的任何转移。使用Fisher精确检验筛选与寡转移或广泛颅外疾病有统计学关联(p<0.1)的突变。生成寡转移疾病可能性的风险评分,并将其与患有寡转移疾病与广泛转移疾病的可能性相关联。对于寡转移患者,进行竞争风险分析以评估寡转移进展的累积发生率。使用Cox回归确定寡转移风险评分与寡进展之间的关联。
130名患者符合研究标准并纳入分析。51名患者(39%)患有颅外寡转移疾病。Guardant检测板中与寡转移疾病存在相关(p<0.1)的基因突变包括ATM、JAK2、MAP2K2和NTRK1,而ARID1A和CCNE1与广泛转移疾病相关。寡转移疾病风险评分为阳性、中性和阴性的患者发生寡转移疾病的可能性分别为78%、41%和11.5%(p<0.0001)。寡转移疾病风险评分为阳性、中性和阴性的患者在6个月时的总生存率分别为86%、82%和64%(p=0.2)。基于Wald卡方检验,寡转移风险评分与寡进展的可能性显著相关。寡转移疾病风险评分为阳性、中性和阴性的患者在6个月时寡转移进展的累积发生率分别为77%、35%和33%(p=0.03)。
对于NSCLC患者,从非侵入性液体活检中阐明颅外寡转移疾病的基因组特征似乎是可行的。具有这种特征的患者早期寡进展发生率较高。外部验证可能会产生一种有潜力指导寡转移患者局部治疗的生物标志物。