Deri Connor R, Moehring Rebekah W, Turner Nicholas A, Spivey Justin, Advani Sonali D, Wrenn Rebekah H, Yarrington Michael E
Department of Pharmacy, Duke University Medical Center, Durham, NC, USA.
Duke Center for Antimicrobial Stewardship and Infection Prevention, Durham, NC, USA.
Antimicrob Steward Healthc Epidemiol. 2024 Oct 3;4(1):e158. doi: 10.1017/ash.2024.437. eCollection 2024.
We aimed to determine whether automated identification of antibiotic targeting suspected urinary tract infection (UTI) shortened the time to antimicrobial stewardship (AS) intervention.
Retrospective before-and-after study.
Tertiary and quaternary care academic medical center.
Emergency department (ED) or admitted adult patients meeting best practice alert (BPA) criteria during pre- and post-BPA periods.
We developed a BPA to alert AS pharmacists of potential ASB triggered by the following criteria: ED or admitted status, antibiotic order with genitourinary indication, and a preceding urinalysis with ≤ 10 WBC/hpf. We evaluated the median time from antibiotic order to AS intervention and overall percent of UTI-related interventions among patients in pre-BPA (01/2020-12/2020) and post-BPA (04/15/2021-04/30/2022) periods.
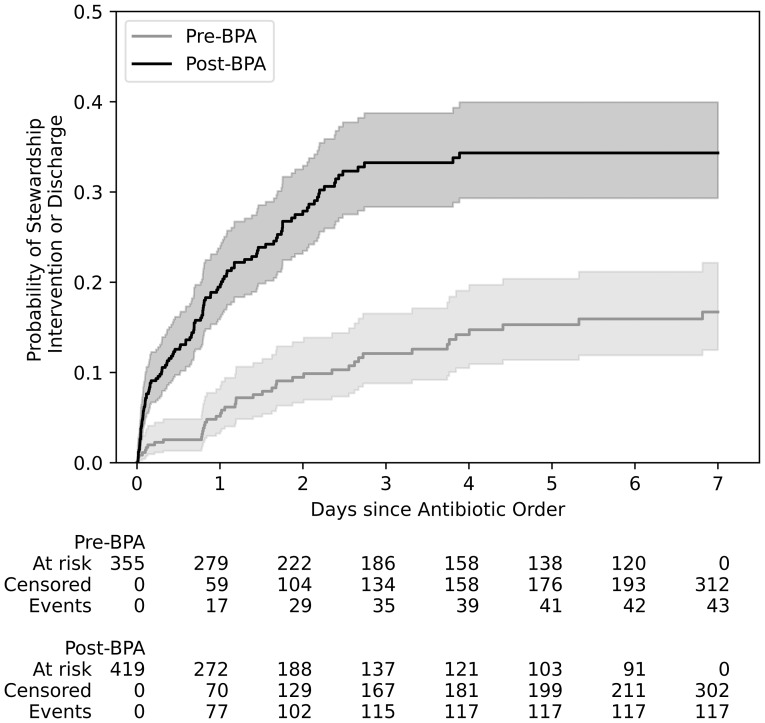
774 antibiotic orders met inclusion criteria: 355 in the pre- and 419 in the post-BPA group. 43 (35 UTI-related) pre-BPA and 117 (94 UTI-related) post-BPA interventions were documented. The median time to intervention was 28 hours (IQR 18-65) in the pre-BPA group compared to 16 hours (IQR 2-34) in the post-BPA group ( < 0.01). Despite absent pyuria, there were six cases with gram-negative bacteremia presumably from a urinary source.
Automated identification of antibiotics targeting UTI without pyuria on urinalysis reduced the time to stewardship intervention and increased the rate of UTI-specific interventions. Clinical decision support aided in the efficiency of AS review and syndrome-targeted impact, but cases still required AS clinical review.
我们旨在确定自动识别针对疑似尿路感染(UTI)的抗生素是否能缩短抗菌药物管理(AS)干预的时间。
回顾性前后对照研究。
三级和四级医疗学术医学中心。
在实施最佳实践警报(BPA)之前和之后期间,符合BPA标准的急诊科(ED)或住院成年患者。
我们制定了一项BPA,以提醒AS药剂师注意由以下标准引发的潜在ASB:ED或住院状态、有泌尿生殖系统指征的抗生素医嘱,以及之前尿分析白细胞≤10个/高倍视野。我们评估了在BPA实施前(2020年1月至2020年12月)和BPA实施后(2021年4月15日至2022年4月30日)期间,患者从抗生素医嘱到AS干预的中位时间以及UTI相关干预的总体百分比。
774份抗生素医嘱符合纳入标准:BPA实施前组355份,BPA实施后组419份。记录了43次(35次与UTI相关)BPA实施前干预和117次(94次与UTI相关)BPA实施后干预。BPA实施前组干预的中位时间为28小时(四分位间距18 - 65),而BPA实施后组为16小时(四分位间距2 - 34)(P<0.01)。尽管无脓尿,但有6例革兰阴性菌血症病例可能源于泌尿生殖道。
自动识别针对尿分析无脓尿的UTI的抗生素可缩短管理干预时间,并提高UTI特异性干预率。临床决策支持有助于提高AS审查效率和综合征针对性影响,但病例仍需AS临床审查。