Department of Anesthesia and Critical Care Medicine, AP-HP, Hôpital Lariboisière, Paris, France.
INSERM, MASCOT, U942, Université Paris Cité, Paris, France.
BMC Med Ethics. 2024 Oct 9;25(1):110. doi: 10.1186/s12910-024-01093-1.
The development of controlled donation after circulatory death (cDCD) is both important and challenging. The tension between end-of-life care and organ donation raises significant ethical issues for healthcare professionals in the intensive care unit (ICU). The aim of this prospective, multicenter, observational study is to better understand ICU physicians' and nurses' experiences with cDCD.
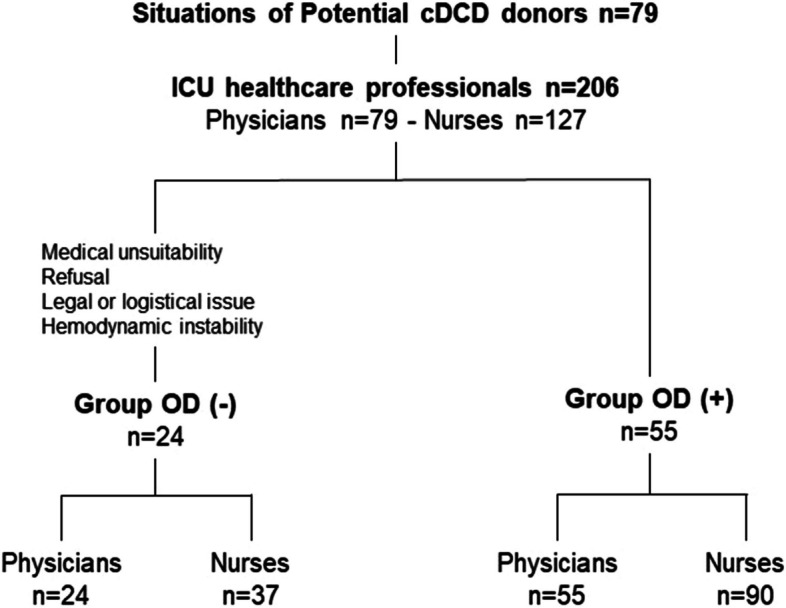
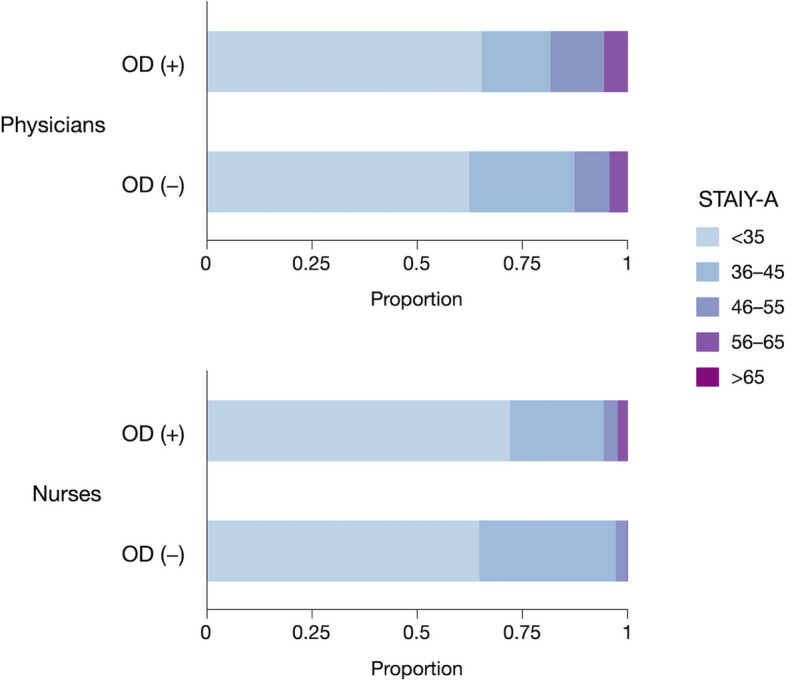
In 32 ICUs in France, ICU physicians and nurses were invited to complete a questionnaire after the death of end-of-life ICU patients identified as potential cDCD donors who had either experienced the withdrawal of life-sustaining therapies alone or with planned organ donation (OD(-) and OD( +) groups). The primary objective was to assess their anxiety (State Anxiety Inventory STAI Y-A) following the death of a potential cDCD donor. Secondary objectives were to explore potential tensions experienced between end-of-life care and organ donation.
Two hundred six ICU healthcare professionals (79 physicians and 127 nurses) were included in the course of 79 potential cDCD donor situations. STAI Y-A did not differ between the OD(-) and OD( +) groups for either physicians or nurses (STAI Y-A were 34 (27-38) in OD(-) vs. 32 (27-40) in OD( +), p = 0.911, for physicians and 32 (25-37) in OD(-) vs. 39 (26-37) in OD( +), p = 0.875, for nurses). The possibility of organ donation was a factor influencing the WLST decision for nurses only, and a factor influencing the WLST implementation for both nurses and physicians. cDCD experience is perceived positively by ICU healthcare professionals overall.
cDCD does not increase anxiety in ICU healthcare professionals compared to other situations of WLST. WLST and cDCD procedures could further be improved by supporting professionals in making their intentions clear between end-of-life support and the success of organ donation, and when needed, by enhancing communication between ICU physician and nurses.
This research was registered in ClinicalTrials.gov (Identifier: NCT05041023, September 10, 2021).
制定循环死亡后控制供体(cDCD)方案十分重要,但也极具挑战性。在重症监护病房(ICU)中,生命末期护理与器官捐献之间的紧张关系给医护人员带来了重大的伦理问题。本前瞻性、多中心、观察性研究旨在深入了解 ICU 医生和护士对 cDCD 的经验。
在法国的 32 家 ICU 中,邀请 ICU 医生和护士在生命末期 ICU 患者死亡后完成问卷,这些患者被认为是潜在的 cDCD 供体,他们要么单独经历了生命支持疗法的撤除,要么经历了计划中的器官捐献(OD(-) 和 OD(+) 组)。主要目的是评估他们在潜在 cDCD 供体死亡后焦虑程度(状态焦虑量表 STAI Y-A)。次要目标是探讨生命末期护理与器官捐献之间潜在的紧张关系。
在 79 例潜在 cDCD 供体情况下,共纳入 206 名 ICU 医护人员(79 名医生和 127 名护士)。OD(-)和 OD(+)组的医生和护士的 STAI Y-A 无差异(OD(-)的 STAI Y-A 为 34(27-38),OD(+)为 32(27-40),p=0.911;OD(-)的 STAI Y-A 为 32(25-37),OD(+)为 39(26-37),p=0.875)。器官捐献的可能性是影响护士 WLST 决策的一个因素,也是影响护士和医生 WLST 实施的一个因素。总的来说,cDCD 经验受到 ICU 医护人员的积极评价。
与其他 WLST 情况相比,cDCD 不会增加 ICU 医护人员的焦虑。通过明确生命末期支持与器官捐献成功之间的意图,并在必要时加强 ICU 医生和护士之间的沟通,可进一步改进 WLST 和 cDCD 程序。
本研究在 ClinicalTrials.gov 注册(标识符:NCT05041023,2021 年 9 月 10 日)。