Intensive Care Unit, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou, People's Republic of China.
Department of Pharmacy, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou, People's Republic of China.
Drug Des Devel Ther. 2024 Oct 5;18:4459-4469. doi: 10.2147/DDDT.S473080. eCollection 2024.
Tigecycline is considered one of the last resorts for treating infections caused by multidrug-resistant bacteria. Continuous renal replacement therapy (CRRT) is widely used in critically ill patients, especially those with acute kidney injury or severe infections. However, pharmacokinetic data for tigecycline in patients receiving CRRT are limited.
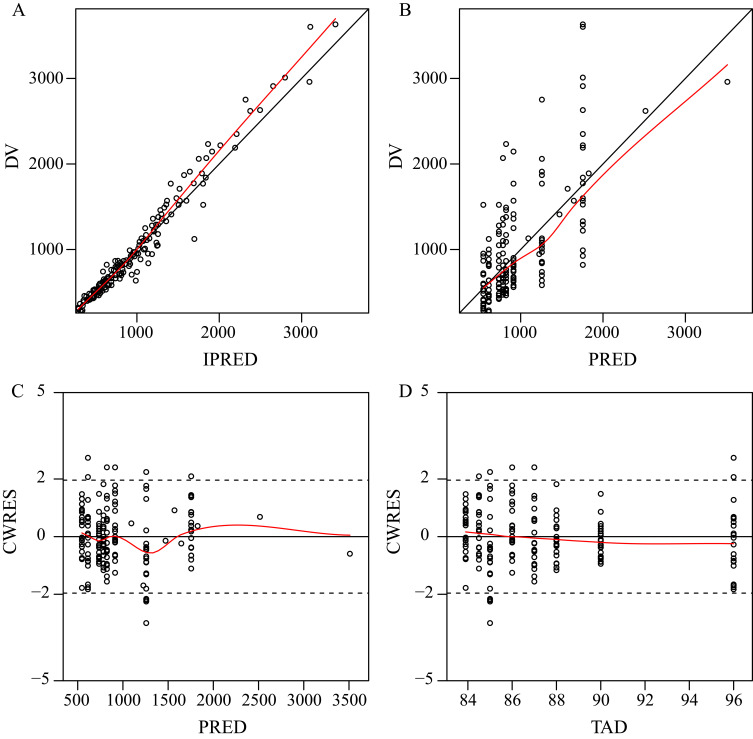
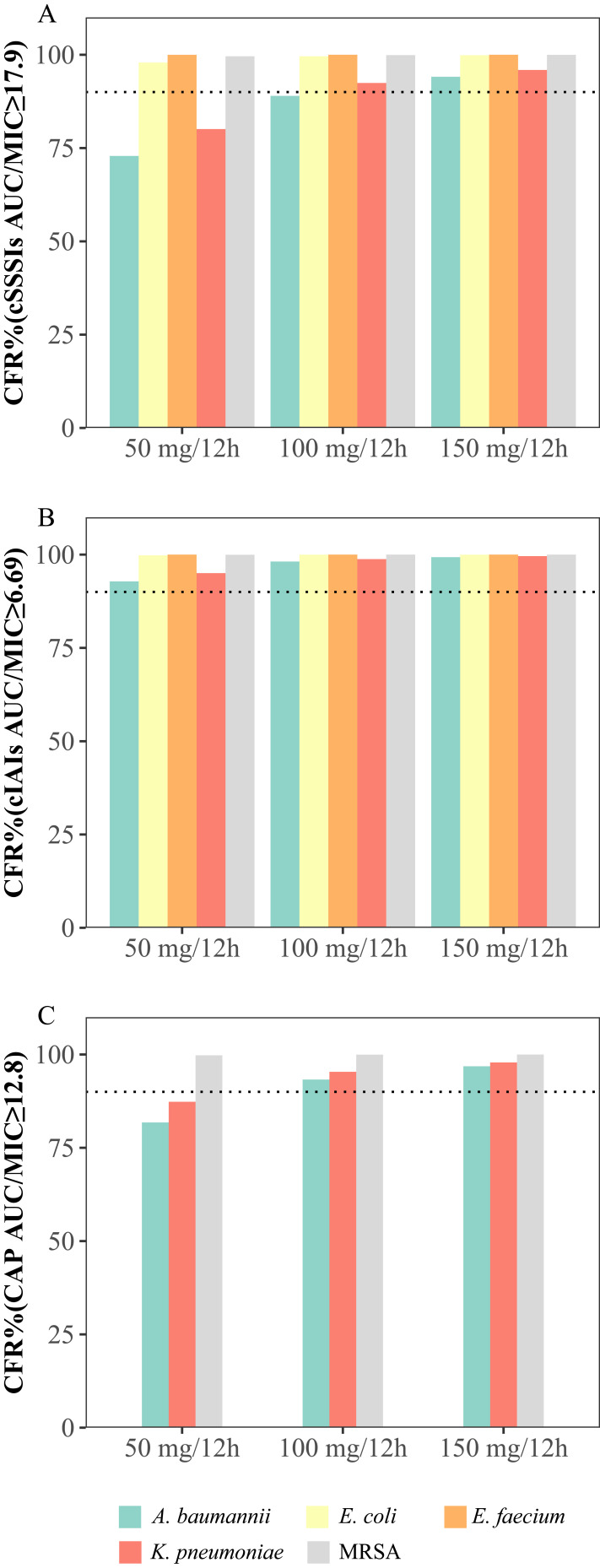
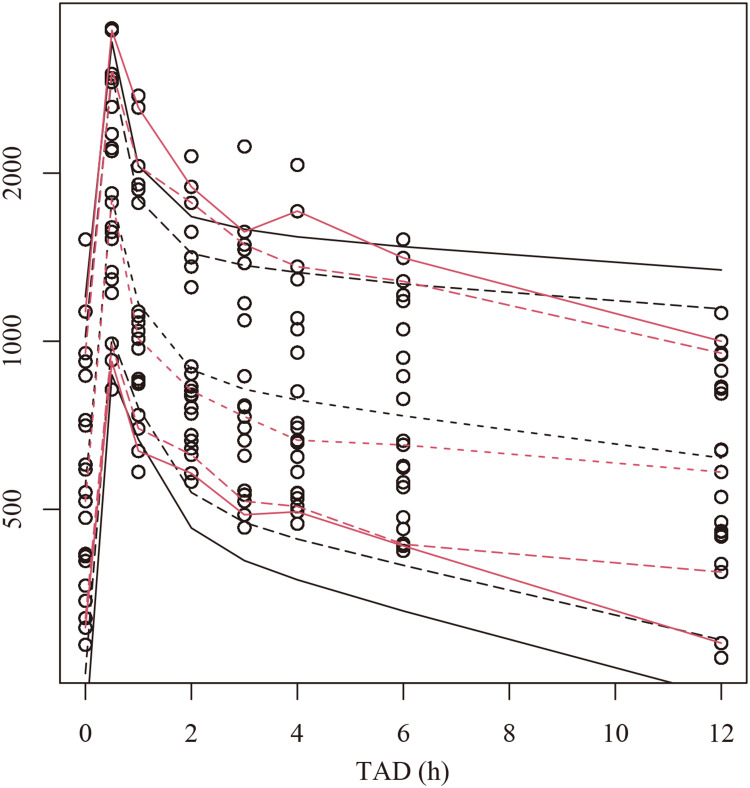
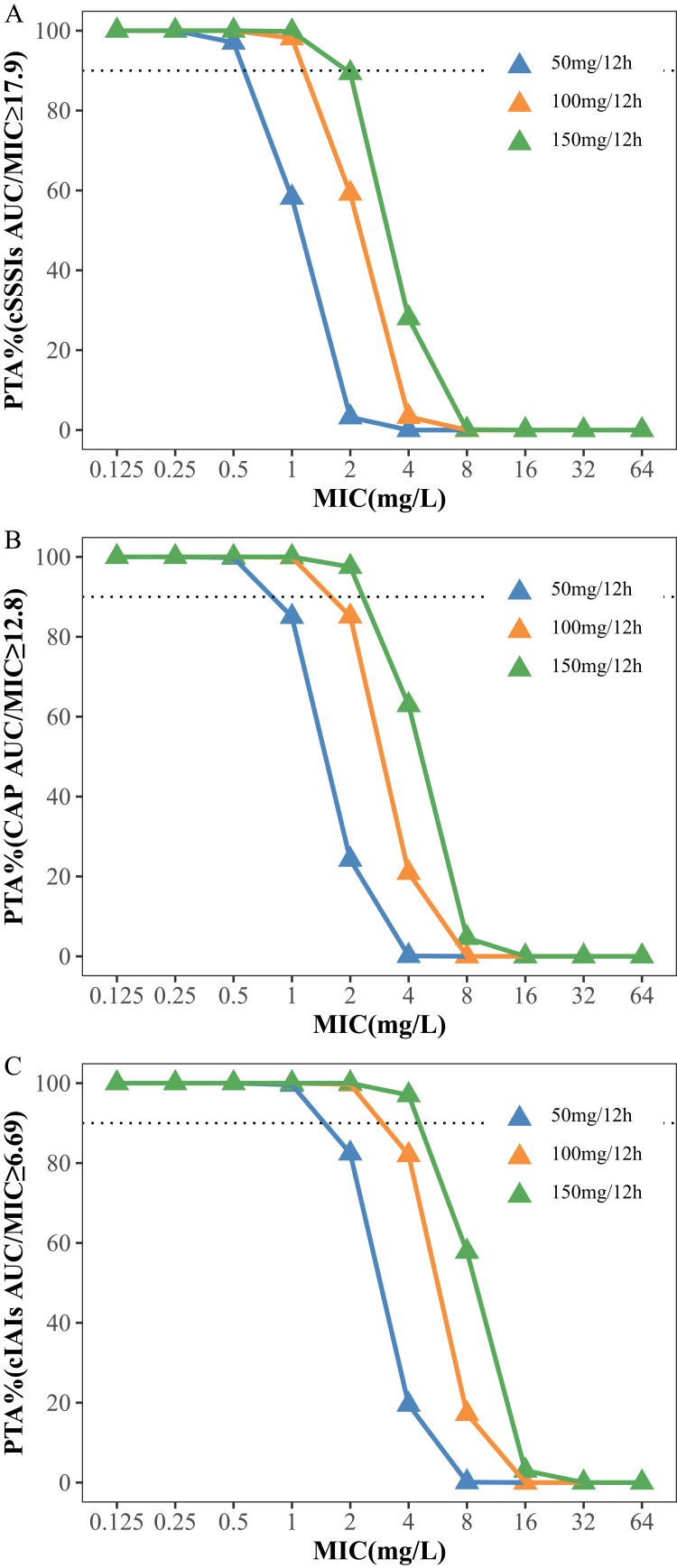
This was a single-center prospective clinical study with intensive sampling that included critically ill patients who received tigecycline and CRRT. A population pharmacokinetic (PPK) model was developed and evaluated by goodness-of-fit plots, bootstrap analysis, visual predictive checks, and numerical predictive checks. Pharmacokinetic/pharmacodynamic target attainment and cumulative fraction of response analyses were performed to explore the potential need for dose adjustments of tigecycline in CRRT.
In total, 21 patients with 167 concentrations were included. A two-compartment model adequately described the tigecycline concentration-time points, but no covariates were found to adequately explain the viability in the pharmacokinetic parameters of tigecycline. The typical values of CL, Q, V1 and V2 were 4.42 L/h, 34.8 L/h, 30.9 L and 98.7 L, respectively. For most infections, the standard regimen of 50 mg/12 h was deemed appropriate, expect for skin and soft skin tissue infections and community-acquired pneumonia caused by and , which required a dosage regimen of 100 mg/12 h or higher.
A tigecycline PPK model describing critically ill patients undergoing CRRT was successfully developed. The optimized dosage regimens for various infections are recommended.
替加环素被认为是治疗多重耐药菌引起的感染的最后手段之一。连续肾脏替代疗法(CRRT)广泛应用于重症患者,尤其是急性肾损伤或严重感染患者。然而,接受 CRRT 的患者替加环素的药代动力学数据有限。
这是一项单中心前瞻性临床研究,采用密集采样,包括接受替加环素和 CRRT 的重症患者。通过拟合度图、bootstrap 分析、可视化预测检查和数值预测检查来建立和评估群体药代动力学(PPK)模型。进行药代动力学/药效学目标达成和累积反应分数分析,以探讨 CRRT 中替加环素剂量调整的潜在需求。
共纳入 21 例患者,采集了 167 个浓度值。两室模型能够充分描述替加环素浓度时间点,但未发现任何协变量能够充分解释替加环素药代动力学参数的变异性。CL、Q、V1 和 V2 的典型值分别为 4.42 L/h、34.8 L/h、30.9 L 和 98.7 L。对于大多数感染,标准剂量 50 mg/12 h 被认为是合适的,除了皮肤和软组织感染以及由 和 引起的社区获得性肺炎,需要 100 mg/12 h 或更高的剂量方案。
成功建立了描述接受 CRRT 的重症患者的替加环素 PPK 模型。推荐了各种感染的优化剂量方案。