Zheng Patricia, Scheffler Aaron, Ewing Susan, Hue Trisha, Jones Sara, Morshed Saam, Mehling Wolf, Torres-Espin Abel, Galivanche Anoop, Lotz Jeffrey, Peterson Thomas, O'Neill Conor
Department of Orthopaedic Surgery, University of California, San Francisco.
Department of Epidemiology and Biostatistics, University of California, San Francisco.
medRxiv. 2024 Sep 27:2024.09.23.24314235. doi: 10.1101/2024.09.23.24314235.
There are a number of risk factors- from biological, psychological, and social domains- for non-specific chronic low back pain (cLBP). Many cLBP treatments target risk factors on the assumption that the targeted factor is not just associated with cLBP but is also a cause (i.e, a causal risk factor). In most cases this is a strong assumption, primarily due to the possibility of confounding variables. False assumptions about the causal relationships between risk factors and cLBP likely contribute to the generally marginal results from cLBP treatments.
The objectives of this study were to a) using rigorous confounding control compare associations between modifiable causal risk factors identified by Mendelian randomization (MR) studies with associations in a cLBP population and b) estimate the association of these risk factors with cLBP outcomes.
STUDY DESIGN/SETTING: Cross sectional analysis of a longitudinal, online, observational study.
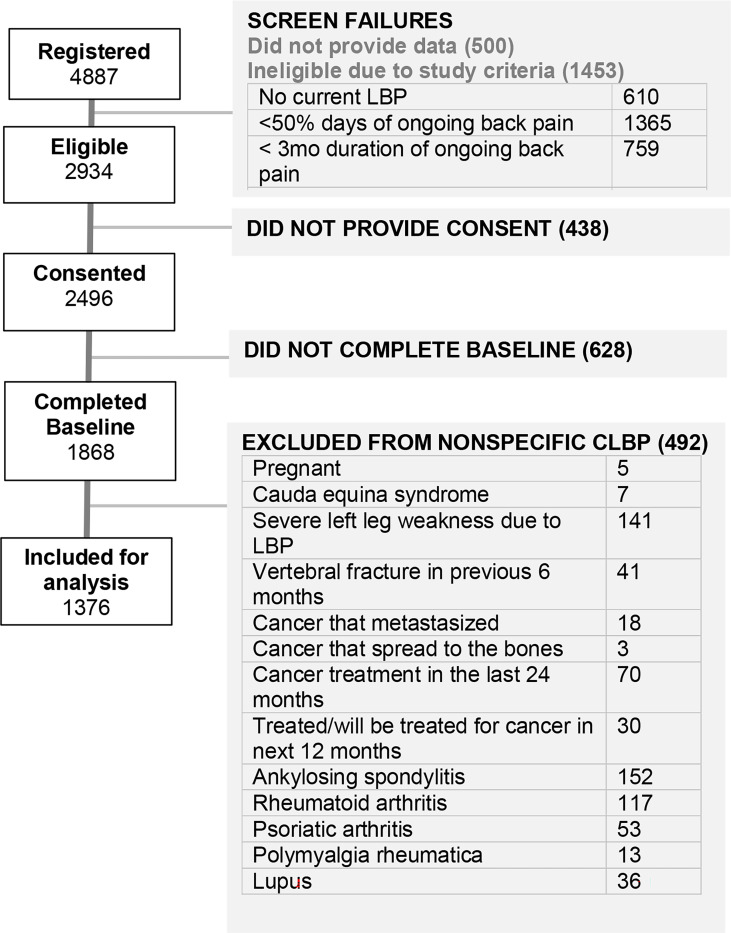
1,376 participants in BACKHOME, a longitudinal observational e-Cohort of U.S. adults with cLBP that is part of the NIH Back Pain Consortium (BACPAC) Research Program.
Pain, Enjoyment of Life, and General Activity (PEG) Scale.
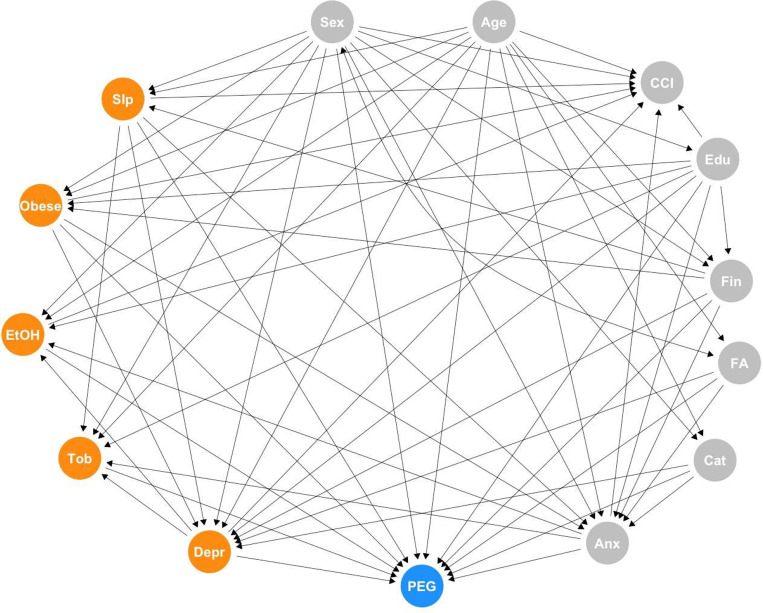
Five risk factors were selected based on evidence from MR randomization studies: sleep disturbance, depression, BMI, alcohol use, and smoking status. Confounders were identified using the ESC-DAG approach, a rigorous method for building directed acyclic graphs based on causal criteria. Strong evidence for confounding was found for age, female sex, education, relationship status, financial strain, anxiety, fear avoidance and catastrophizing. These variables were used to determine the adjustment sets for the primary analysis. Potential confounders with weaker evidence were used for a sensitivity analysis.
Participants had the following characteristics: age 54.9 ± 14.4 years, 67.4% female, 60% never smokers, 29.9% overweight, 39.5% obese, PROMIS sleep disturbance T-score 54.8 ± 8.0, PROMIS depression T-score 52.6 ± 10.1, Fear-avoidance Beliefs Questionnaire 11.6 ± 5.9, Patient Catastrophizing Scale 4.5 ± 2.6, PEG 4.4 ± 2.2. In the adjusted models alcohol use, sleep disturbance, depression, and obesity were associated with PEG, after adjusting for confounding variables identified via a DAG constructed using a rigorous protocol. The adjusted effect estimates- the expected change in the PEG outcome for every standard deviation increase or decrease in the exposure (or category shift for categorical exposures) were the largest for sleep disturbance and obesity. Each SD increase in the PROMIS sleep disturbance T-score resulted in a mean 0.77 (95% CI: 0.66, 0.88) point increase in baseline PEG score. Compared to participants with normal BMI, adjusted mean PEG score was slightly higher by 0.37 points (95% CI: 0.09, 0.65) for overweight participants, about 0.8 to 0.9 points higher for those in obesity classes I and II, and 1.39 (95% CI: 0.98, 1.80) points higher for the most obese participants. Each SD increase in the PROMIS depression T-score was associated with a mean 0.28 (95% CI: 0.17, 0.40) point increase in baseline PEG score, while each SD decrease in number of alcoholic drinks per week resulted in a mean 0.12 (95%CI: 0.01, 0.23) increase in baseline PEG score in the adjusted model.
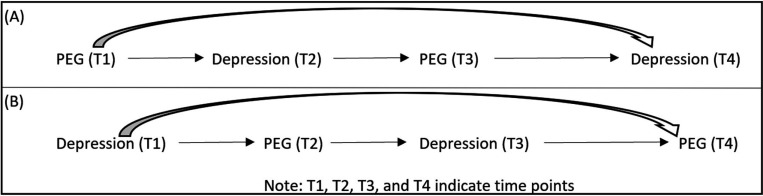
Several modifiable causal risk factors for cLBP - alcohol use, sleep disturbance, depression, and obesity- are associated with PEG, after adjusting for confounding variables identified via a DAG constructed using a rigorous protocol. Convergence of our findings for sleep disturbance, depression, and obesity with the results from MR studies, which have different designs and biases, strengthens the evidence for causal relationships between these risk factors and cLBP (1). The estimated effect of change in a risk factors on change in PEG were the largest for sleep disturbance and obesity. Future analyses will evaluate these relationships with longitudinal data.
非特异性慢性下腰痛(cLBP)存在许多来自生物、心理和社会领域的风险因素。许多cLBP治疗针对风险因素,其假设是目标因素不仅与cLBP相关,而且是一个原因(即因果风险因素)。在大多数情况下,这是一个强有力的假设,主要是由于存在混杂变量的可能性。关于风险因素与cLBP之间因果关系的错误假设可能导致cLBP治疗的总体效果一般很有限。
本研究的目的是:a)使用严格的混杂控制,比较孟德尔随机化(MR)研究确定的可改变因果风险因素与cLBP人群中的关联;b)估计这些风险因素与cLBP结局的关联。
研究设计/设置:对一项纵向在线观察性研究进行横断面分析。
BACKHOME研究中的1376名参与者,BACKHOME是美国患有cLBP的成年人的纵向观察性电子队列,是美国国立卫生研究院背痛联盟(BACPAC)研究项目的一部分。
疼痛、生活满意度和日常活动(PEG)量表。
根据MR随机化研究的证据选择五个风险因素:睡眠障碍、抑郁、体重指数(BMI)、饮酒和吸烟状况。使用ESC-DAG方法识别混杂因素,这是一种基于因果标准构建有向无环图的严格方法。发现年龄、女性性别、教育程度、恋爱状况、经济压力、焦虑、恐惧回避和灾难化思维等因素存在强烈的混杂证据。这些变量用于确定主要分析的调整集。证据较弱的潜在混杂因素用于敏感性分析。
参与者具有以下特征:年龄54.9±14.4岁,67.4%为女性,60%从不吸烟,29.9%超重,39.5%肥胖,PROMIS睡眠障碍T评分54.8±8.0,PROMIS抑郁T评分52.6±10.1,恐惧回避信念问卷评分11.6±5.9,患者灾难化思维量表评分4.5±2.6,PEG评分4.4±2.2。在调整模型中,在通过严格方案构建的有向无环图识别的混杂变量进行调整后,饮酒、睡眠障碍、抑郁和肥胖与PEG相关。调整后的效应估计值——暴露每增加或减少一个标准差(或分类暴露的类别变化)时PEG结局的预期变化——在睡眠障碍和肥胖方面最大。PROMIS睡眠障碍T评分每增加一个标准差,基线PEG评分平均增加0.77(95%置信区间:0.66,0.88)分。与BMI正常的参与者相比,超重参与者的调整后平均PEG评分略高0.37分(95%置信区间:0.09,0.65),I级和II级肥胖参与者高约0.8至0.9分,最肥胖参与者高1.39(95%置信区间:0.98,1.80)分。PROMIS抑郁T评分每增加一个标准差,基线PEG评分平均增加0.28(95%置信区间:0.17,0.40)分,而在调整模型中,每周饮酒量每减少一个标准差,基线PEG评分平均增加0.12(95%置信区间:0.01,0.23)分。
在通过严格方案构建的有向无环图识别的混杂变量进行调整后,cLBP的几个可改变因果风险因素——饮酒、睡眠障碍、抑郁和肥胖——与PEG相关。我们关于睡眠障碍、抑郁和肥胖的研究结果与设计和偏差不同的MR研究结果的一致性,加强了这些风险因素与cLBP之间因果关系的证据。风险因素变化对PEG变化的估计效应在睡眠障碍和肥胖方面最大。未来的分析将使用纵向数据评估这些关系。