Messier Stephen P, Monroe Megan G, Callahan Leigh F, Mihalko Shannon L, Beavers Daniel P, Queen Kate, Miller Gary D, Losina Elena, Katz Jeffrey N, Loeser Richard F, DeVita Paul, Hunter David J, Quandt Sara A
Wake Forest University, Winston-Salem, North Carolina.
University of North Carolina at Chapel Hill.
Arthritis Care Res (Hoboken). 2025 Jan;77(1):69-76. doi: 10.1002/acr.25448. Epub 2024 Nov 11.
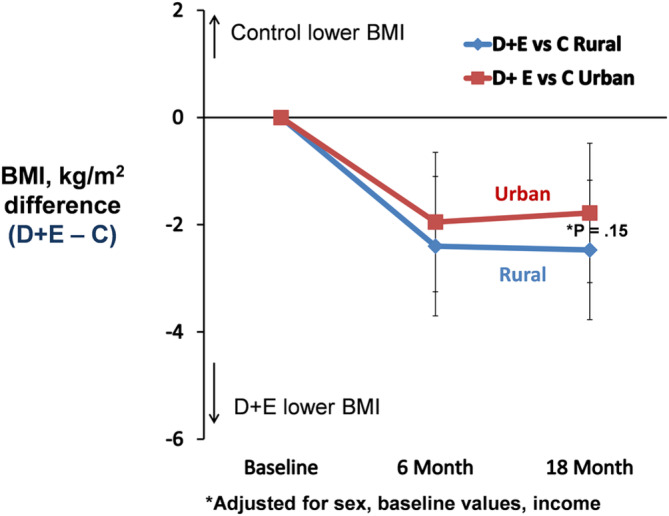
The study objective was to determine whether the clinical response of older adults with knee osteoarthritis and overweight or obesity to 18 months of diet and exercise (D + E) or attention control (C) interventions differed between participants from rural versus urban communities.
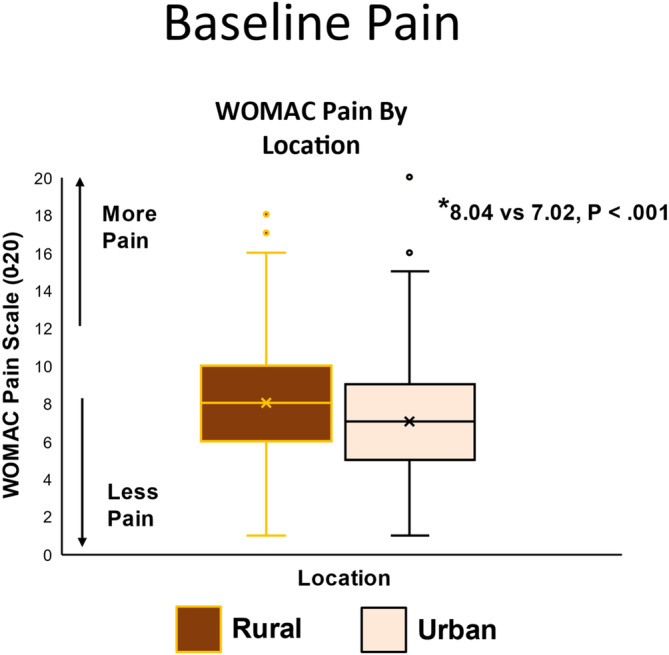
Participants were 823 older adults (mean age, 64.6 years; 77% women) with knee osteoarthritis and overweight or obesity who resided in rural (n = 410) and urban (n = 413) counties in North Carolina. All were enrolled in the Weight Loss and Exercise for Communities with Arthritis in North Carolina clinical trial that randomly assigned participants to either 18 months of D + E or C interventions. General linear models were used to examine differences in clinical outcomes between rural and urban groups after adjusting for covariates.
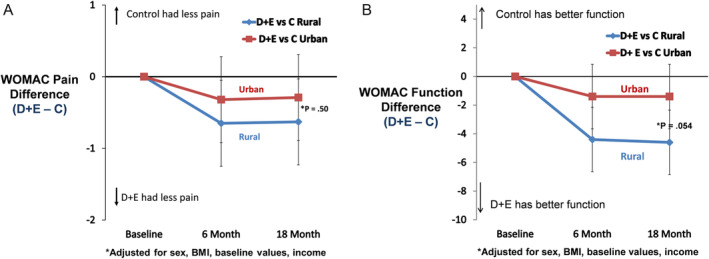
The rural group had significant differences (P < 0.05) at baseline in clinical outcomes, education, comorbidities, medication use, and income compared with the urban dwellers. After adjusting for baseline differences, the group (rural or urban) by treatment (D + E or C) interactions for Western Ontario McMasters Universities Osteoarthritis Index (WOMAC) pain (rural: D + E - C = -0.63, 95% confidence interval [CI] -1.31 to 0.06; urban: D + E - C= -0.29, 95% CI -0.99 to 0.41; P = 0.50) and WOMAC function (rural: D + E - C = -4.60, 95% CI -6.89 to -2.31; urban: D + E - C = -1.38, 95% CI -3.73 to 0.94; P = 0.054) indicated that the groups responded similarly to the interventions.
Among participants with knee osteoarthritis and overweight or obesity, D + E compared to C led to similar pain outcomes in rural and urban dwellers that favored D + E. The possibility that there may be greater differential efficacy in functional outcomes among rural participants needs further study.
本研究的目的是确定患有膝关节骨关节炎且超重或肥胖的老年人,在接受18个月的饮食和运动(D + E)或注意力控制(C)干预后,农村社区与城市社区参与者的临床反应是否存在差异。
参与者为823名患有膝关节骨关节炎且超重或肥胖的老年人(平均年龄64.6岁;77%为女性),他们居住在北卡罗来纳州的农村(n = 410)和城市(n = 413)县。所有参与者均参加了北卡罗来纳州关节炎社区减肥与运动临床试验,该试验将参与者随机分配至接受18个月的D + E或C干预。在调整协变量后,使用一般线性模型检查农村和城市组之间临床结果的差异。
与城市居民相比,农村组在基线时的临床结果、教育程度、合并症、药物使用和收入方面存在显著差异(P < 0.05)。在调整基线差异后,按治疗(D + E或C)分组(农村或城市)的西部安大略麦克马斯特大学骨关节炎指数(WOMAC)疼痛交互作用(农村:D + E - C = -0.63,95%置信区间[CI] -1.31至0.06;城市:D + E - C = -0.29,95% CI -0.99至0.41;P = 0.50)和WOMAC功能交互作用(农村:D + E - C = -4.60,95% CI -6.89至-2.31;城市:D + E - C = -1.38,95% CI -3.73至0.94;P = 0.054)表明两组对干预的反应相似。
在患有膝关节骨关节炎且超重或肥胖的参与者中,与C相比,D + E在农村和城市居民中导致了相似的疼痛结果,且更有利于D + E。农村参与者在功能结果方面可能存在更大差异疗效的可能性需要进一步研究。