Department of Anesthesiology and Perioperative Medicine, University of Rochester School of Medicine, Rochester, New York.
Department of Public Health Sciences, University of Rochester School of Medicine, Rochester, New York.
JAMA Netw Open. 2024 Oct 1;7(10):e2438563. doi: 10.1001/jamanetworkopen.2024.38563.
Marginalized populations have been disproportionately affected by the COVID-19 pandemic. Critically ill patients belonging to racial and ethnic minority populations treated in hospitals operating under crisis or near-crisis conditions may have experienced worse outcomes than White individuals.
To examine whether hospital strain was associated with worse outcomes for older patients hospitalized with sepsis and whether these increases in poor outcomes were greater for members of racial and ethnic minority groups compared with White individuals.
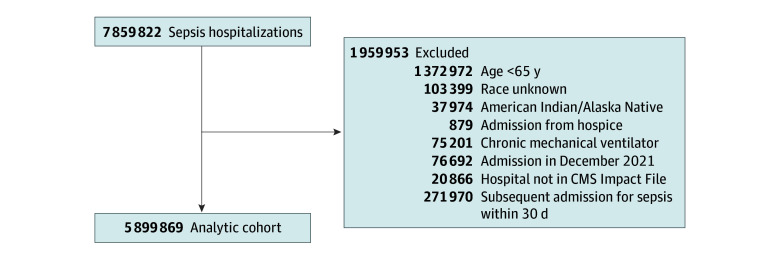
DESIGN, SETTING, AND PARTICIPANTS: In this cross-sectional study, multivariable regression analysis was conducted to assess differential changes in all-cause 30-day mortality and major morbidity among older racial and ethnic minoritized individuals hospitalized with sepsis compared with White individuals and changes in hospital strain using Medicare claims data. Data were obtained on patients hospitalized between January 1, 2016, and December 31, 2021, and analyzed between December 16, 2023, and July 11, 2024.
Time-varying weekly hospital percentage of inpatients with COVID-19.
Composite of all-cause 30-day mortality and major morbidity.
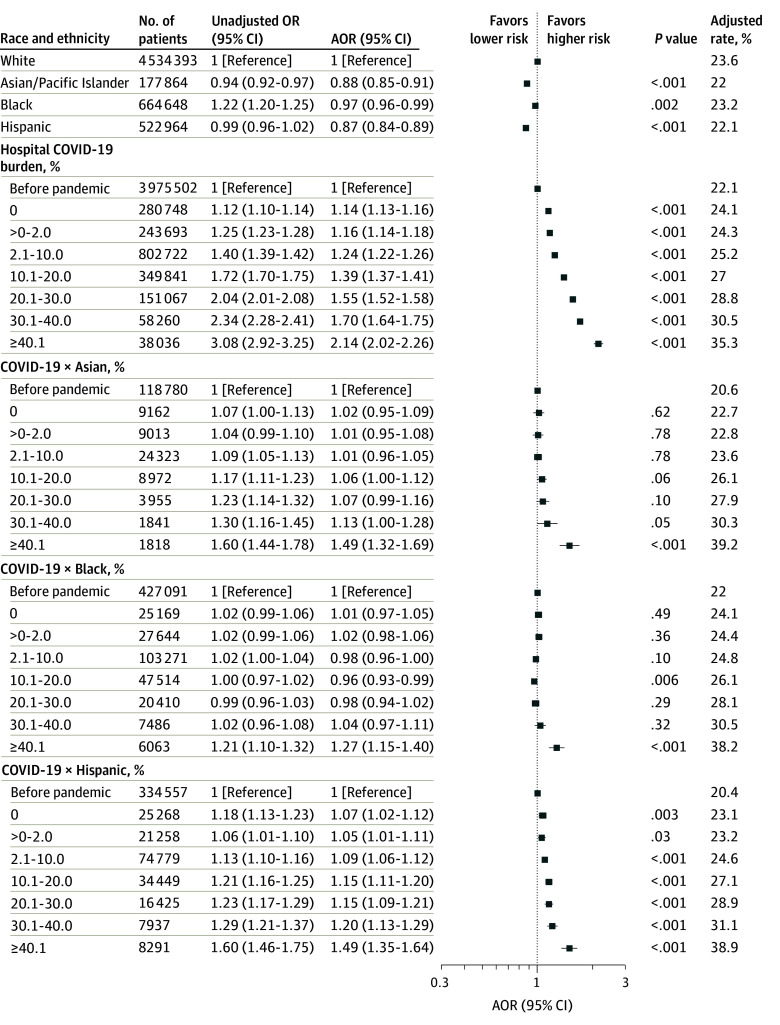
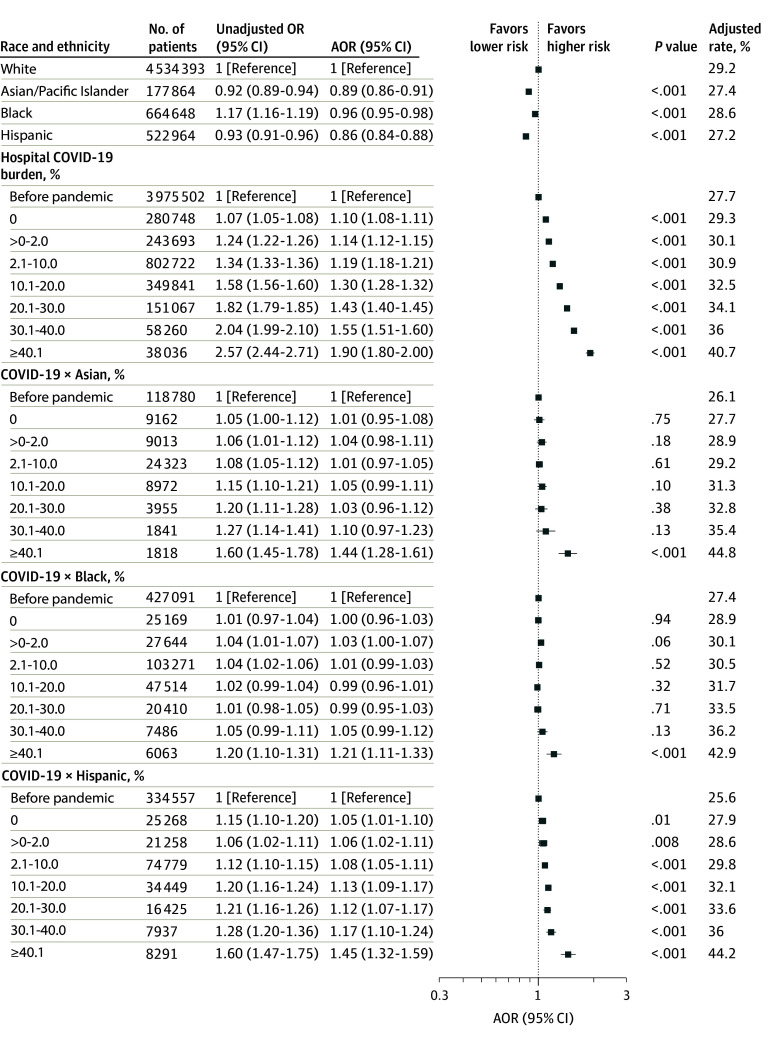
Among the 5 899 869 hospitalizations for sepsis (51.5% women; mean [SD] age, 78.2 [8.8] years), there were 177 864 (3.0%) Asian, 664 648 (11.3%) Black, 522 964 (8.9%) Hispanic, and 4 534 393 (76.9%) White individuals. During weeks when the hospital COVID-19 burden was greater than 40%, the risk of death or major morbidity increased nearly 2-fold (adjusted odds ratio [AOR], 1.90; 95% CI, 1.80-2.00; P < .001) for White individuals compared with before the pandemic. Asian, Black, and Hispanic individuals experienced 44% (AOR, 1.44; 95% CI, 1.28-1.61; P < .001), 21% (AOR, 1.21; 95% CI, 1.11-1.33; P < .001), and 45% (AOR, 1.45; 95% CI, 1.32-1.59; P < .001) higher risk of death or morbidity, respectively, compared with White individuals when the hospital weekly COVID-19 burden was greater than 40%.
In this cross-sectional study, older adults hospitalized with sepsis were more likely to die or experience major morbidity as the hospital COVID-19 burden increased. These increases in adverse outcomes were greater in magnitude among members of minority populations than for White individuals.
边缘化人群受到 COVID-19 大流行的不成比例的影响。在处于危机或接近危机状态下运作的医院中接受治疗的属于少数族裔和种族的危重病患者,其结局可能比白人患者更差。
检查医院压力是否与老年脓毒症患者的预后较差有关,以及与白人患者相比,少数族裔患者的这些不良结局增加是否更大。
设计、地点和参与者:在这项横断面研究中,使用医疗保险索赔数据进行多变量回归分析,以评估与白人患者相比,老年脓毒症患者住院期间全因 30 天死亡率和主要发病率的差异变化,以及医院压力的变化。数据来自于 2016 年 1 月 1 日至 2021 年 12 月 31 日期间住院的患者,分析于 2023 年 12 月 16 日至 2024 年 7 月 11 日之间进行。
每周医院 COVID-19 住院患者的百分比。
全因 30 天死亡率和主要发病率的复合指标。
在 5899869 例脓毒症住院患者中(51.5%为女性;平均[SD]年龄为 78.2[8.8]岁),有 177864 例(3.0%)为亚洲人,664648 例(11.3%)为黑人,522964 例(8.9%)为西班牙裔,4534393 例(76.9%)为白人。在医院 COVID-19 负担超过 40%的几周内,与大流行前相比,白人患者死亡或出现主要并发症的风险几乎增加了两倍(调整后的优势比 [AOR],1.90;95%置信区间 [CI],1.80-2.00;P<0.001)。与白人患者相比,亚洲人、黑人、西班牙裔患者的死亡或发病风险分别增加了 44%(AOR,1.44;95%CI,1.28-1.61;P<0.001)、21%(AOR,1.21;95%CI,1.11-1.33;P<0.001)和 45%(AOR,1.45;95%CI,1.32-1.59;P<0.001)。
在这项横断面研究中,随着医院 COVID-19 负担的增加,患有脓毒症的老年患者更有可能死亡或出现主要并发症。与白人患者相比,少数族裔患者的这些不良结局增加幅度更大。