Jiang Yuxin, Liu Tao, Xu Ke, Cheng Qinpei, Lu Wanjun, Xie Jingyuan, Chen Mo, Li Yu, Du Yanjun, Liang Shuo, Song Yong, Wu Jiang, Lv Tangfeng, Zhan Ping
School of Medicine, Southeast University, Nanjing, China.
Department of Nuclear Medicine, Jinling Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, China.
Transl Lung Cancer Res. 2024 Sep 30;13(9):2236-2253. doi: 10.21037/tlcr-24-291. Epub 2024 Sep 25.
Frequently recurrent malignant pleural effusion (MPE) significantly hampers the life quality of advanced non-small cell lung cancer (NSCLC) patients. We aimed to explore the effects of progression patterns and local intervention on MPE recurrence and apply fluorodeoxyglucose positron emission tomography/computed tomography (F-FDG PET/CT) to establish a predictive model for MPE recurrence in NSCLC.
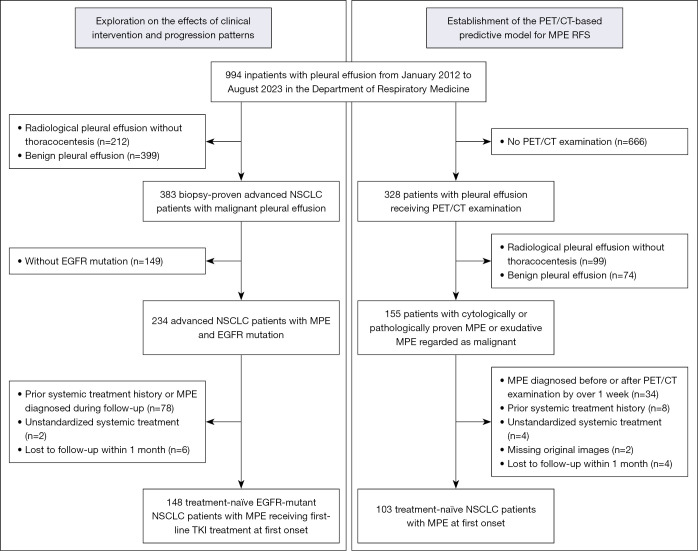
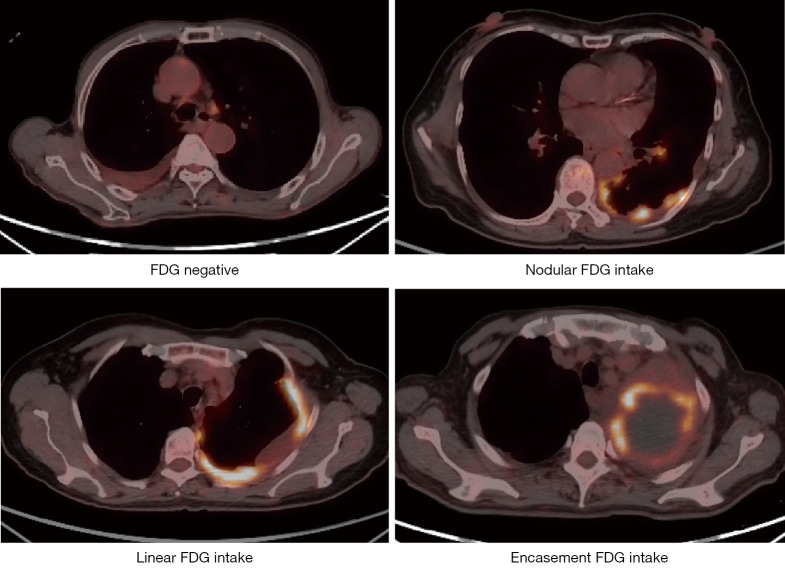
We retrospectively recruited two cohorts of patients including treatment-naïve NSCLC diagnosed with MPE at the onset and receiving PET/CT scanning, as well as those with MPE and undergoing first-line epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitor (TKI) treatment. Pleural maximum standardized uptake value (SUV), metabolic tumor burden (MTV), total lesion glycolysis (TLG), and uptake patterns as well as SUV of lymph nodes (LN) were extracted. The primary outcome was MPE recurrence defined as re-accumulation of cytologically proven ipsilateral MPE. Step-wise multivariate Cox regression was used to identify candidate variables. Cox regression analysis and random survival forest were applied to establish models.
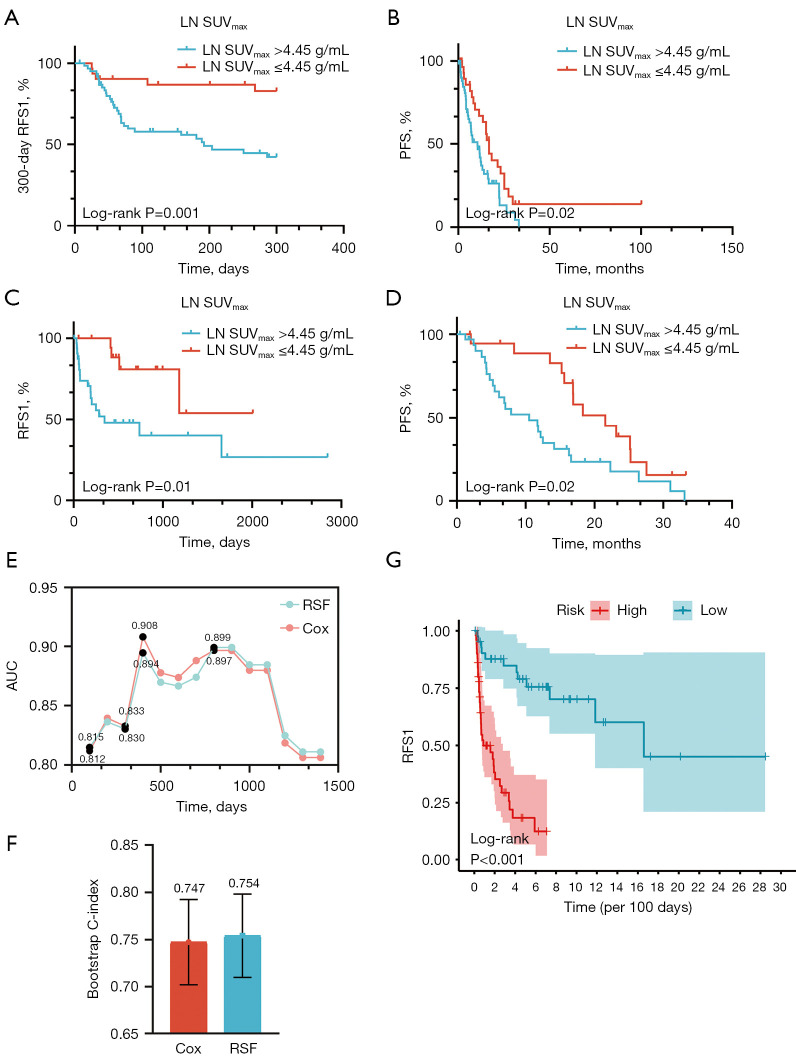
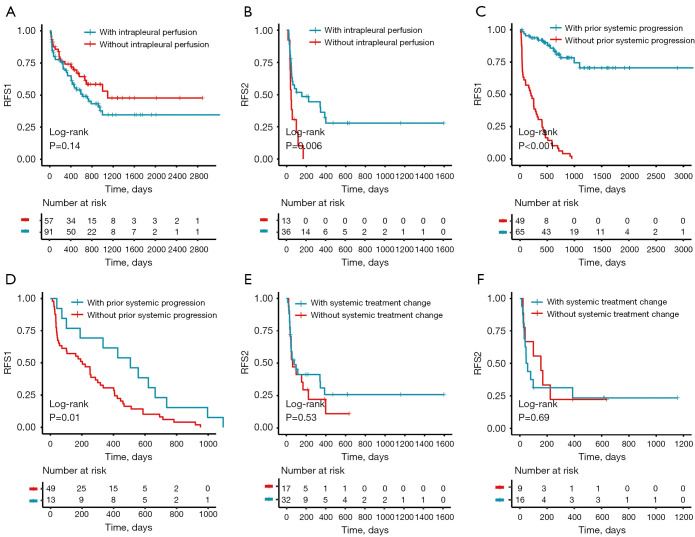
A total of 148 treatment-naïve patients with EGFR-TKI treatment and MPE were recruited during the median follow-up period of 683 days, with 69 (46.6%) and 35 (23.6%) witnessing MPE recurrence at least once and twice. Intrapleural perfusion therapy at first recurrence was a protective factor for the second MPE recurrence (P=0.006), while intrapleural perfusion therapy at baseline could not benefit the first MPE recurrence (P=0.14). Conversely, prior systemic progression indicative of the change of systemic treatment was a protective factor for time to the first MPE recurrence (P<0.001); instead, the change of systemic treatment at the first MPE recurrence was not associated with second MPE recurrence (P=0.53). In another cohort with treatment-naïve NSCLC patients with MPE and PET/CT scanning, 103 patients regardless of the actionable mutation status were recruited during the median follow-up period of 304 days. Multivariate analysis suggested that the LN SUV >4.50 g/mL [hazard ratio (HR), 2.54; P=0.01], female gender (HR, 0.40; P=0.01), bone metastases (HR, 3.16; P=0.001), and systemic treatment (targeted therapy chemotherapy: HR, 0.32; P=0.002; immunotherapy therapy chemotherapy: HR, 0.99; P=0.97) could collectively indicate MPE recurrence with an optimal 300-day area under the curve (AUC) of 0.83. For patients with actionable mutation, LN SUV >4.50 g/mL (P=0.02) could forecast MPE recurrence independently.
In summary, LN rather than pleural metabolic activity or uptake patterns could predict MPE recurrence for patients with or without targeted therapy. We should re-consider the application of intrapleural perfusion treatment for first-onset MPE and prompt it more at the moment of recurrent MPE. Promisingly, we could probably apply the non-invasive tool to identify the risk factors for MPE recurrence.
频繁复发的恶性胸腔积液(MPE)严重影响晚期非小细胞肺癌(NSCLC)患者的生活质量。我们旨在探讨进展模式和局部干预对MPE复发的影响,并应用氟脱氧葡萄糖正电子发射断层扫描/计算机断层扫描(F-FDG PET/CT)建立NSCLC患者MPE复发的预测模型。
我们回顾性招募了两组患者,包括初治时诊断为MPE并接受PET/CT扫描的NSCLC患者,以及患有MPE并接受一线表皮生长因子受体(EGFR)-酪氨酸激酶抑制剂(TKI)治疗的患者。提取胸膜最大标准化摄取值(SUV)、代谢肿瘤体积(MTV)、总病灶糖酵解(TLG)、摄取模式以及淋巴结(LN)的SUV。主要结局为MPE复发,定义为经细胞学证实的同侧MPE再次积聚。采用逐步多因素Cox回归分析确定候选变量,并应用Cox回归分析和随机生存森林建立模型。
在中位随访期683天内,共招募了148例初治且接受EGFR-TKI治疗并伴有MPE的患者,其中69例(46.6%)和35例(23.6%)至少经历过一次和两次MPE复发。首次复发时进行胸腔内灌注治疗是第二次MPE复发的保护因素(P=0.006),而基线时进行胸腔内灌注治疗对首次MPE复发无益处(P=0.14)。相反,提示全身治疗改变的既往全身进展是首次MPE复发时间的保护因素(P<0.001);而首次MPE复发时全身治疗的改变与第二次MPE复发无关(P=0.53)。在另一组初治且伴有MPE并接受PET/CT扫描的NSCLC患者中,在中位随访期304天内招募了103例患者,无论其可操作突变状态如何。多因素分析表明,LN SUV>4.50 g/mL[风险比(HR),2.54;P=0.01]、女性(HR,0.40;P=0.01)、骨转移(HR,3.16;P=0.001)和全身治疗(靶向治疗+化疗:HR,0.32;P=0.002;免疫治疗+化疗:HR,0.99;P=0.97)可共同提示MPE复发,最佳曲线下面积(AUC)在300天时为0.83。对于具有可操作突变的患者,LN SUV>4.50 g/mL(P=0.02)可独立预测MPE复发。
总之,对于接受或未接受靶向治疗的患者,LN而非胸膜代谢活性或摄取模式可预测MPE复发。我们应重新考虑首次发生MPE时胸腔内灌注治疗的应用,并在MPE复发时更积极地进行该治疗。有望地,我们可能应用这种非侵入性工具来识别MPE复发的危险因素。