Lipid Clinic, Department of Endocrinology, Morbid Obesity and Preventive Medicine, Oslo University Hospital 0424, Oslo, Norway.
Department of Clinical Science and Education, Södersjukhuset, Karolinska Institutet 118 83, Stockholm, Sweden.
J Diabetes Res. 2024 Oct 12;2024:6142211. doi: 10.1155/2024/6142211. eCollection 2024.
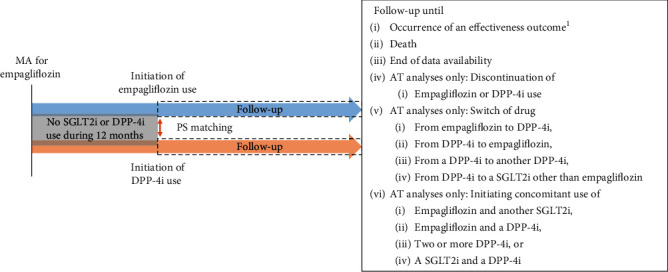
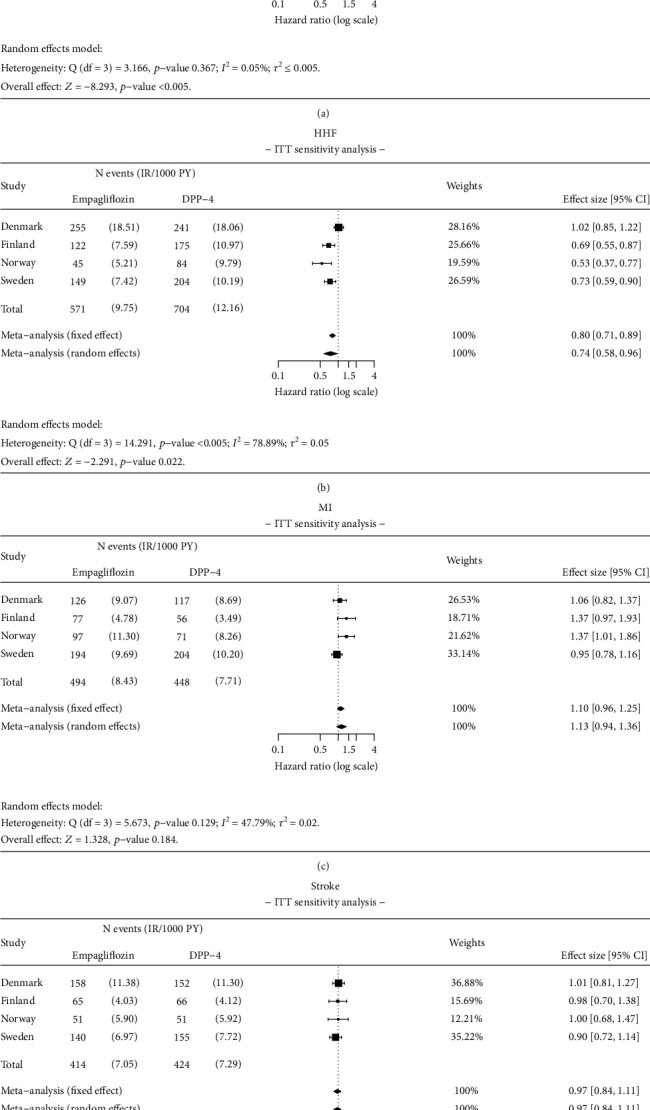
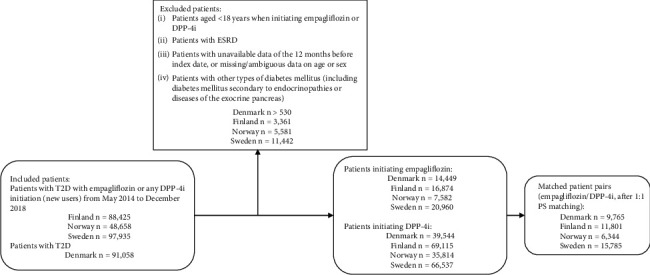
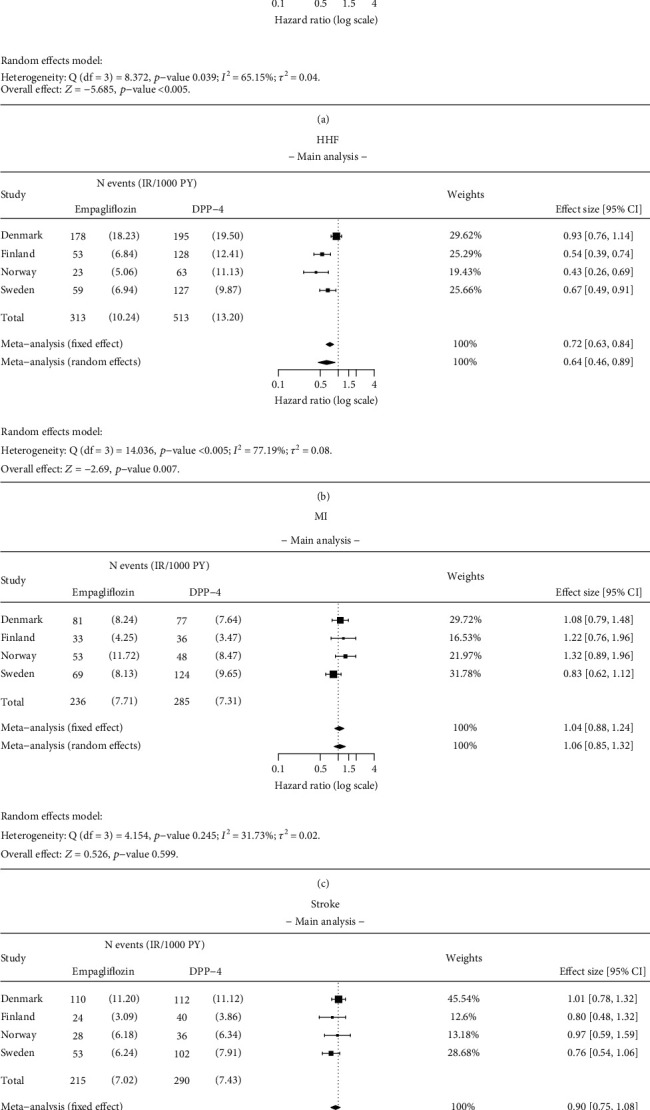
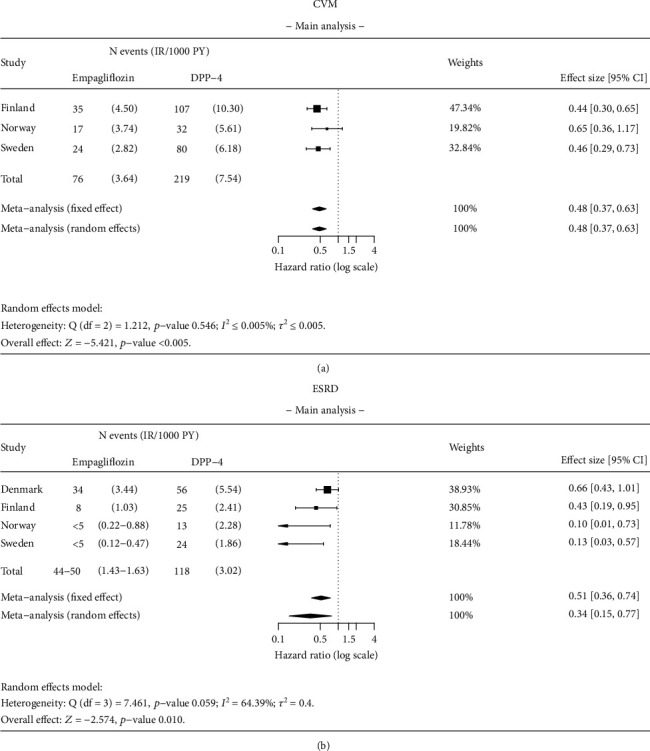
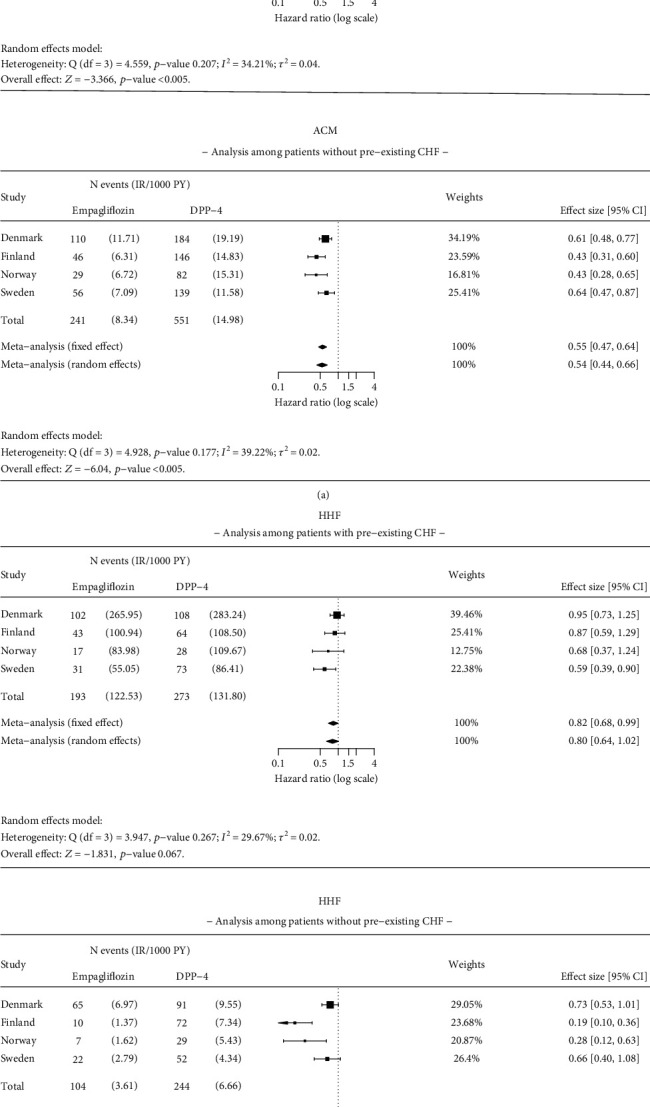
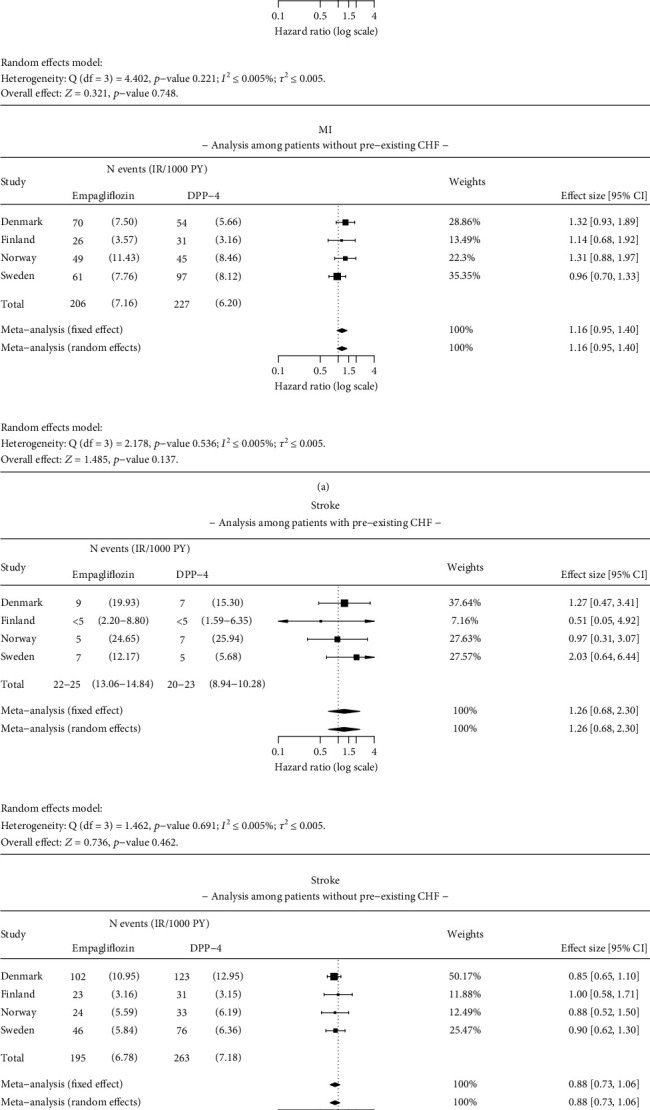
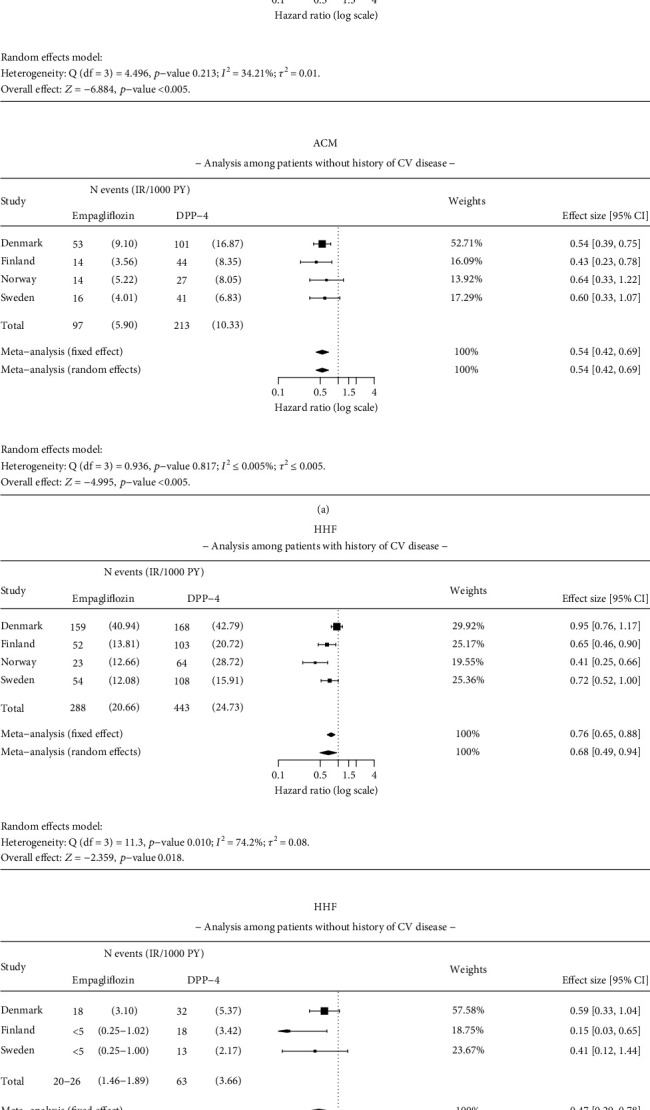
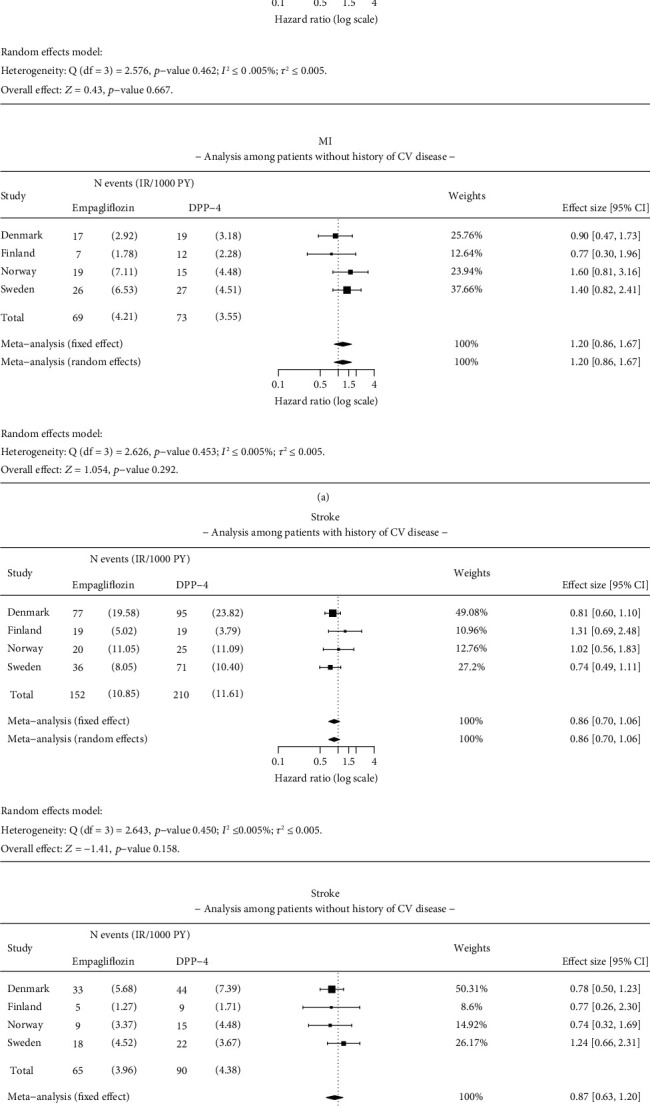
: To evaluate the effectiveness of empagliflozin in reducing all-cause mortality (ACM), hospitalization for heart failure (HHF), myocardial infarction (MI), stroke, cardiovascular mortality (CVM), and end-stage renal disease (ESRD) in routine clinical practice in the Nordic countries of the Empagliflozin Comparative Effectiveness and Safety (EMPRISE) study. : This noninterventional, multicountry cohort study used secondary data from four Nordic countries (Denmark, Sweden, Finland, and Norway). Propensity score (PS) matched (1:1) adults with type 2 diabetes (T2D) initiating empagliflozin (a sodium-glucose cotransporter-2 inhibitor) during 2014-2018 who were compared to those initiating a dipeptidyl peptidase-4 inhibitor (DPP-4i). Cox proportional hazards regression modelling was used to assess the risk for ACM, HHF, MI, stroke, CVM, and ESRD. Meta-analyses were conducted and hazard ratios (HRs) with 95% confidence intervals (CIs) from random-effects models were calculated. : A total of 43,695 pairs of PS-matched patients were identified. Patients initiating empagliflozin exhibited a 49% significantly lower risk of ACM (HR: 0.51, 95% CI 0.40-0.64) compared to DPP-4i. Additionally, empagliflozin was associated with a 36% significantly lower risk of HHF (HR: 0.64, 95% CI 0.46-0.89), a 52% significantly lower risk of CVM (HR: 0.48, 95% CI 0.37-0.63), and a 66% significantly lower risk of ESRD (HR: 0.34, 95% CI 0.15-0.77) compared to DPP-4i. No significant differences were observed in the risk of stroke and MI between patients initiating empagliflozin compared with those initiating a DPP-4i. Results were generally consistent for subgroups (with/without pre-existing CV disease or congestive heart failure) and in sensitivity analyses. : Empagliflozin initiation was associated with a significantly reduced risk of ACM, HHF, CVM, and ESRD compared with initiation of DPP-4i in patients with T2D when examining routine clinical practice data from Nordic countries.
评估恩格列净在降低全因死亡率(ACM)、心力衰竭住院(HHF)、心肌梗死(MI)、卒中和心血管死亡率(CVM)以及终末期肾病(ESRD)方面的有效性在北欧国家的 Empagliflozin 比较疗效和安全性(EMPRISE)研究中,在常规临床实践中。这项非干预性、多国队列研究使用了来自四个北欧国家(丹麦、瑞典、芬兰和挪威)的二级数据。2014-2018 年期间,使用倾向评分(PS)匹配(1:1)接受钠-葡萄糖共转运蛋白 2 抑制剂(SGLT2i)恩格列净治疗的 2 型糖尿病(T2D)成年患者,并与接受二肽基肽酶-4 抑制剂(DPP-4i)的患者进行比较。采用 Cox 比例风险回归模型评估 ACM、HHF、MI、卒中和 CVM 和 ESRD 的风险。进行了荟萃分析,并计算了来自随机效应模型的危险比(HR)和 95%置信区间(CI)。
共确定了 43695 对 PS 匹配的患者。与 DPP-4i 相比,接受恩格列净治疗的患者 ACM 的风险显著降低 49%(HR:0.51,95%CI 0.40-0.64)。此外,与 DPP-4i 相比,恩格列净治疗与 HHF(HR:0.64,95%CI 0.46-0.89)、CVM(HR:0.48,95%CI 0.37-0.63)和 ESRD(HR:0.34,95%CI 0.15-0.77)的风险显著降低 66%。与接受 DPP-4i 的患者相比,接受恩格列净治疗的患者在卒中和 MI 的风险无显著差异。在亚组(伴或不伴预先存在的 CV 疾病或充血性心力衰竭)和敏感性分析中,结果基本一致。
在检查来自北欧国家的常规临床实践数据时,与接受 DPP-4i 治疗的患者相比,接受恩格列净治疗的患者的 ACM、HHF、CVM 和 ESRD 风险显著降低。