Department of Thoracic Surgery, The Affiliated Lihuili Hospital, Ningbo University, Ningbo, 315000, China.
Health Science Center, Ningbo University, Ningbo, 315000, China.
Sci Rep. 2024 Oct 23;14(1):25111. doi: 10.1038/s41598-024-76230-2.
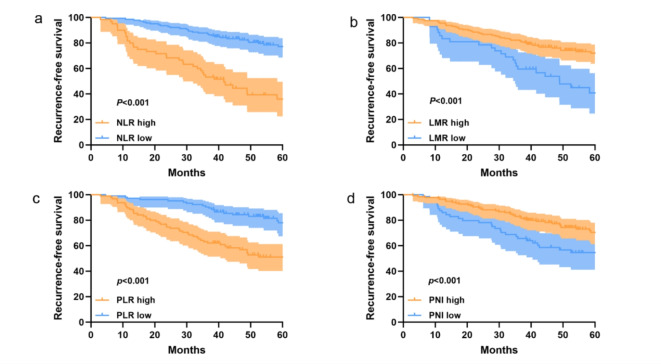
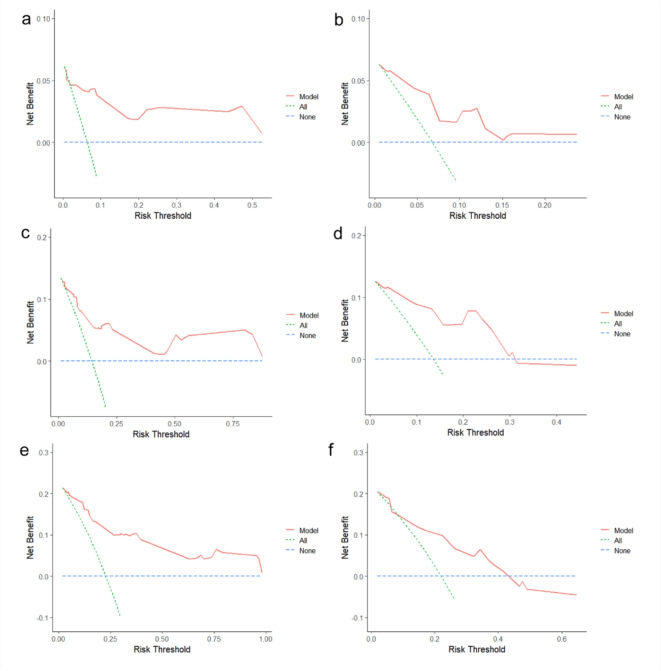
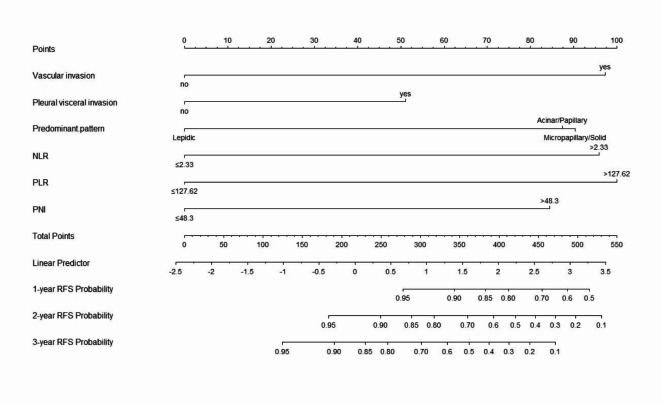
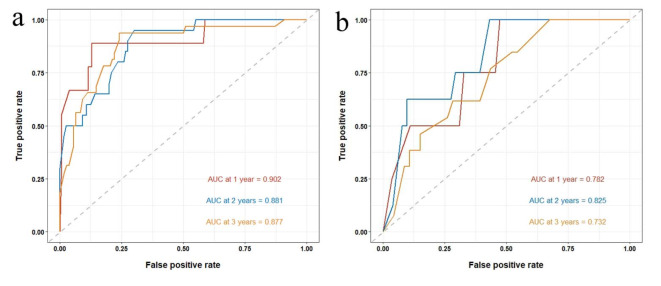
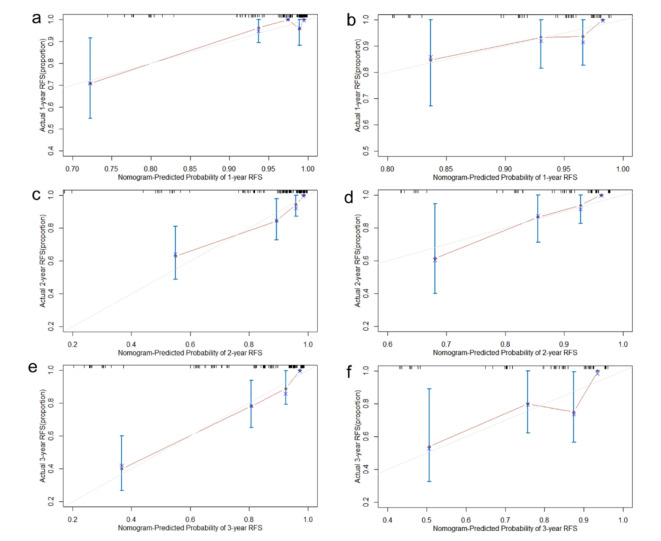
To explore the inflammation-nutrition indices and related clinical factors affecting early recurrence in patients with stage IB LUAD. A retrospective analysis was conducted on clinical and pathological data of patients diagnosed with stage IB LUAD who underwent radical surgery in our hospital from January 2016 to January 2021. Using R software, patients were randomly divided into training (n = 140) and validation (n = 59) cohorts in a 7:3 ratio. Univariate and multivariate Cox regression analyses were performed to identify risk factors for RFS and construct a predictive model. The performance of the model was evaluated using the area under the receiver operating characteristic curve (AUC), concordance index (C-index), and calibration curve. Clinical utility of the model was assessed using decision curve analysis (DCA). Multivariate Cox regression analysis revealed that vascular invasion, visceral pleural invasion, predominant pattern, preoperative NLR > 2.33, preoperative PLR > 127.62, and preoperative PNI ≤ 48.3 were independent risk factors for RFS. The C-index of the nomogram model constructed based on these independent risk factors was 0.825 (95% CI: 0.762-0.881) in the training cohort and 0.772 (95% CI: 0.667-0.876) in the validation cohort. The ROC curves showed AUCs of 0.902, 0.881, and 0.877 for 1-year, 2-year, and 3-year RFS in the training cohort and AUCs of 0.782, 0.825, and 0.732 in the validation cohort respectively. Calibration curve and decision curve analysis indicated good clinical value of the model. The nomogram model based on inflammation-nutrition indices has predictive value for early recurrence in patients with stage IB LUAD.
探讨影响 IB 期 LUAD 患者早期复发的炎症-营养指数及相关临床因素。对 2016 年 1 月至 2021 年 1 月在我院接受根治性手术治疗的 IB 期 LUAD 患者的临床和病理资料进行回顾性分析。采用 R 软件,以 7:3 的比例将患者随机分为训练集(n=140)和验证集(n=59)。采用单因素和多因素 Cox 回归分析识别 RFS 的危险因素,并构建预测模型。采用受试者工作特征曲线下面积(AUC)、一致性指数(C 指数)和校准曲线评估模型性能。采用决策曲线分析(DCA)评估模型的临床实用性。多因素 Cox 回归分析显示,血管侵犯、脏层胸膜侵犯、主要模式、术前 NLR>2.33、术前 PLR>127.62 和术前 PNI≤48.3 是 RFS 的独立危险因素。基于这些独立危险因素构建的列线图模型在训练队列中的 C 指数为 0.825(95%CI:0.762-0.881),在验证队列中的 C 指数为 0.772(95%CI:0.667-0.876)。ROC 曲线显示,训练队列中 1 年、2 年和 3 年 RFS 的 AUC 分别为 0.902、0.881 和 0.877,验证队列中的 AUC 分别为 0.782、0.825 和 0.732。校准曲线和决策曲线分析表明该模型具有良好的临床价值。基于炎症-营养指数的列线图模型对 IB 期 LUAD 患者的早期复发具有预测价值。