Sciacca Vanessa, Sohns Christian, Crijns Harry J G M, Marrouche Nassir F, Schramm Rene, Moersdorf Maximilian, Fink Thomas, Bergau Leonard, Hindricks Gerhard, Dagres Nikolaos, Sossalla Samuel, Costard-Jaeckle Angelika, Fox Henrik, El Hamriti Mustapha, Konietschke Frank, Rudolph Volker, Gummert Jan, Tijssen Jan G P, Sommer Philipp
Clinic for Electrophysiology, Herz- und Diabeteszentrum NRW, Ruhr-Universität Bochum, Bad Oeynhausen, Germany.
Department of Cardiology and CARIM, Maastricht University, Cardiovascular Research Institute Maastricht, Maastricht, The Netherlands.
Eur J Heart Fail. 2025 Feb;27(2):255-263. doi: 10.1002/ejhf.3505. Epub 2024 Oct 24.
The CASTLE-HTx trial showed the benefit of atrial fibrillation (AF) ablation compared to medical therapy in decreasing mortality, need for left ventricular assist device implantation or heart transplantation (HTx) in patients with end-stage heart failure (HF). Herein we describe the effects of catheter ablation on AF burden, arrhythmia recurrences, and ventricular function in end-stage HF.
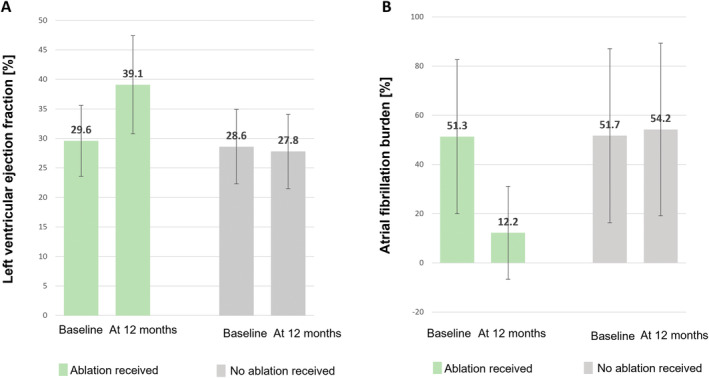
The CASTLE-HTx protocol randomized 194 patients in end-stage HF with AF to catheter ablation and medical therapy or medical therapy alone. AF burden, left ventricular ejection fraction (LVEF), and type of AF were assessed at baseline and at each follow-up visit. Overall, 97 patients received ablation; 66 patients (68%) underwent pulmonary vein isolation (PVI) and 31 patients (32%) were treated with PVI and additional ablation. Electroanatomic mapping showed the extent of left atrial low voltage (cardiomyopathy) >10% in 31 (31.9%) patients. At 12 months post-ablation, persistent AF was present in 31/89 patients (34.8%), which was significantly less frequent compared to baseline (p = 0.0001). Median AF burden reduction was 36.3 (interquartile range 13.6-63.3) percentage points at 12 months and LVEF improved from 29.2 ± 6.2% to 39.1 ± 8.3% (p < 0.001) following ablation. AF burden reduction <50% was significantly associated with LVEF improvement ≥5% at 12 months after ablation (p = 0.017).
Atrial fibrillation ablation in end-stage HF leads to a substantial decrease in AF burden, a regression from persistent to paroxysmal AF and notably improved LVEF. Favourable ablation outcomes were observed in patients regardless of the presence or absence of signs indicating left atrial cardiomyopathy.
CASTLE-HTx试验表明,对于终末期心力衰竭(HF)患者,与药物治疗相比,房颤(AF)消融术在降低死亡率、减少左心室辅助装置植入或心脏移植(HTx)需求方面具有益处。在此,我们描述导管消融术对终末期HF患者房颤负荷、心律失常复发及心室功能的影响。
CASTLE-HTx方案将194例终末期HF合并AF患者随机分为导管消融联合药物治疗组或单纯药物治疗组。在基线及每次随访时评估房颤负荷、左心室射血分数(LVEF)及房颤类型。总体而言,97例患者接受了消融治疗;66例患者(68%)接受了肺静脉隔离(PVI),31例患者(32%)接受了PVI及额外消融治疗。电解剖标测显示,31例(31.9%)患者左心房低电压(心肌病)范围>10%。消融术后12个月时,89例患者中有31例(34.8%)存在持续性房颤,与基线相比频率显著降低(p = 0.0001)。消融术后12个月时,房颤负荷中位数降低36.3(四分位间距13.6 - 63.3)个百分点,消融后LVEF从29.2±6.2%改善至39.1±8.3%(p < 0.001)。消融术后12个月时,房颤负荷降低<50%与LVEF改善≥5%显著相关(p = 0.017)。
终末期HF患者的房颤消融术可使房颤负荷大幅降低,使持续性房颤转变为阵发性房颤,并显著改善LVEF。无论有无提示左心房心肌病的体征,患者均观察到良好的消融效果。