Starup-Hansen Joachim, Williams Simon C, Valetopoulou Alexandra, Khan Danyal Z, Horsfall Hugo Layard, Moudgil-Joshi Jigishaa, Burton Oliver, Kanona Hala, Saeed Shakeel R, Muirhead William, Marcus Hani J, Grover Patrick
Victor Horsley Department of Neurosurgery, The National Hospital for Neurology and Neurosurgery, University College London NHS Trust, London, United Kingdom.
Wellcome/EPSRC Centre for Interventional and Surgical Sciences, University College London, London, United Kingdom.
J Neurol Surg B Skull Base. 2024 Jan 22;85(Suppl 2):e131-e144. doi: 10.1055/a-2222-0016. eCollection 2024 Oct.
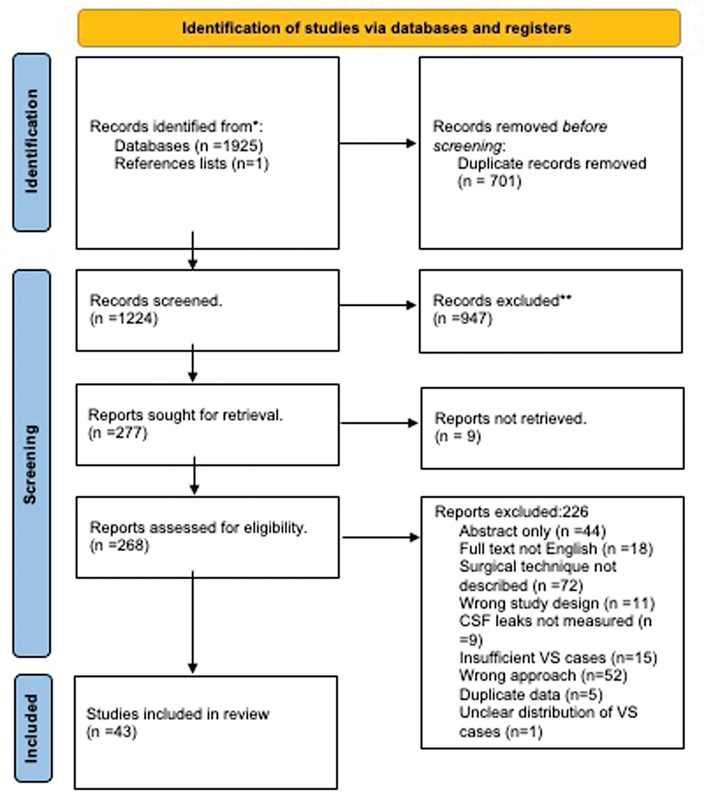
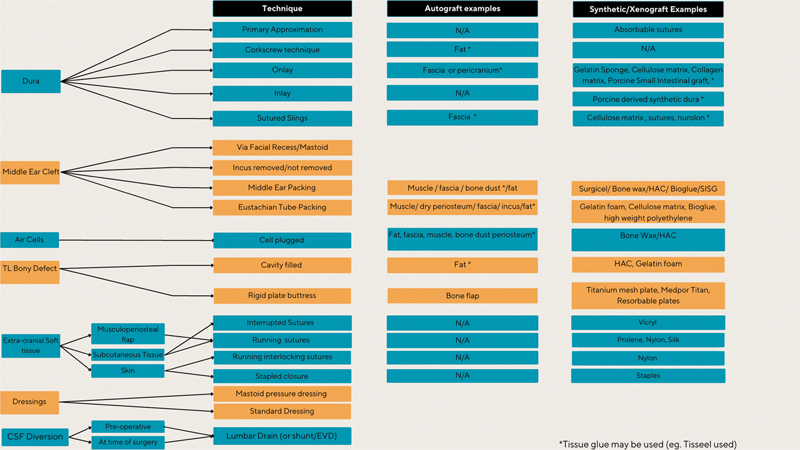
Despite advances in skull base reconstruction techniques, cerebrospinal fluid (CSF) leaks remain a relatively common complication after translabyrinthine (TL) vestibular schwannoma (VS) surgery. We conducted a systematic review to synthesize the repair techniques and materials used in TL VS surgery to prevent CSF leaks. A systematic review of studies published since 2000 reporting techniques to prevent CSF leaks during adult TL VS surgery was conducted. A narrative synthesis of primary repair protocols was produced, and a taxonomy was established. Additionally, the advantages, disadvantages, and associated CSF leak rates of different repair protocols were extracted. All 43 studies were case series, and 39 were retrospective. Repair strategies included heterogeneous combinations of autografts, xenografts, and synthetic materials. A taxonomy was produced, classifying repairs into seven distinct stages, including approaches to the dura, middle ear cleft, air cells, TL bony defect, extra-cranial soft tissue, postoperative dressings, and CSF diversion. The median postoperative incidence of CSF leaks was 6% (interquartile range: 0-10%). This systematic review reveals substantial inter-institutional heterogeneity in intraoperative strategies to prevent CSF leaks following TL VS surgery. However, comparing these techniques is challenging due to the multiple predictive factors for CSF leaks and their inconsistent reporting. We propose a taxonomy of seven stages to classify operative techniques and materials aimed at preventing CSF leaks. We recommend that future evaluations should adopt a prospective approach encompassing data collection strategies that considers all operative stages described by our taxonomy.
尽管颅底重建技术取得了进展,但脑脊液(CSF)漏仍是经迷路(TL)前庭神经鞘瘤(VS)手术后相对常见的并发症。我们进行了一项系统评价,以综合TL VS手术中用于预防脑脊液漏的修复技术和材料。
对2000年以来发表的关于成人TL VS手术中预防脑脊液漏技术的研究进行了系统评价。对主要修复方案进行了叙述性综合,并建立了分类法。此外,还提取了不同修复方案的优缺点及相关脑脊液漏发生率。
所有43项研究均为病例系列,39项为回顾性研究。修复策略包括自体移植物、异种移植物和合成材料的不同组合。制定了一种分类法,将修复分为七个不同阶段,包括硬脑膜、中耳腔、气房、TL骨缺损、颅外软组织、术后敷料和脑脊液分流的处理方法。脑脊液漏的术后中位发生率为6%(四分位间距:0-10%)。
这项系统评价揭示了TL VS手术后预防脑脊液漏的术中策略在机构间存在很大差异。然而,由于脑脊液漏的多种预测因素及其报告不一致,比较这些技术具有挑战性。我们提出了一个七个阶段的分类法,以对旨在预防脑脊液漏的手术技术和材料进行分类。我们建议未来的评估应采用前瞻性方法,包括考虑我们分类法所描述的所有手术阶段的数据收集策略。