Montano Nicola, Signorelli Francesco, Giordano Martina, D'Onofrio Federica Ginevra, Izzo Alessandro, D'Ercole Manuela, Ioannoni Eleonora, Pennisi Giovanni, Caricato Anselmo, Pallini Roberto, Olivi Alessandro
Department of Neurosurgery, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Rome, Italy.
Neurosurgical Intensive Care Unit, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Rome, Italy.
Surg Neurol Int. 2021 Jun 7;12:258. doi: 10.25259/SNI_42_2021. eCollection 2021.
The retrosigmoid approach represents a crucial surgical route to address different lesions in the cerebellopontine angle but cerebrospinal fluid (CSF) leak still remains the most frequent complication after this approach. Here, we analyzed the impact of different factors in CSF leak development after a retrosigmoid approach. Identifying risk factors related to a specific approach may help the surgeon to tailor the perioperative management and to appropriately counsel patients regarding their risk profile.
We retrospectively reviewed the clinical, surgical, and outcome data of 103 consecutive patients (M/F, 47/56; mean follow-up 35.6 ± 23.9 months) who underwent a retrosigmoid approach for different cerebellopontine angle pathologies and studied the impact of different factors on the occurrence of a CSF leak to univariate and multivariate analysis.
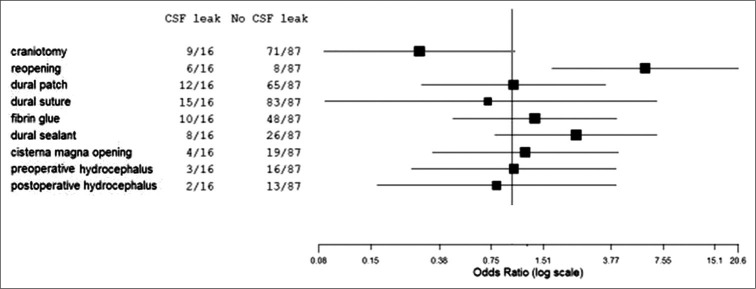
Seventy-nine patients (76.7%) were operated for tumors growing in the cerebellopontine angle. Twenty-four patients (23.2%) underwent microvascular decompression to treat a drug-resistant trigeminal neuralgia. Sixteen patients (15.5%) developed CSF leak in the postoperative course of which six underwent surgical revision. Performing a craniectomy as surgical procedure ( = 0.0450) and performing a reopening procedure (second surgery; = 0.0079) were significantly associated to a higher risk of developing CSF leak. Moreover, performing a reopening procedure emerged as an independent factor for CSF developing on multivariate analysis ( = 0.0156).
Patients submitted to craniectomy and patients who underwent a second surgery showed an higher CSF leak rate. Ongoing improvement of biomaterial technology may help neurosurgeons to prevent this potentially life-threatening complication.
乙状窦后入路是处理桥小脑角区不同病变的重要手术路径,但脑脊液漏仍是该入路术后最常见的并发症。在此,我们分析了乙状窦后入路术后脑脊液漏发生的不同因素的影响。识别与特定入路相关的危险因素可能有助于外科医生调整围手术期管理,并就患者的风险状况给予适当的建议。
我们回顾性分析了103例连续患者(男/女,47/56;平均随访35.6±23.9个月)的临床、手术和结局数据,这些患者因不同的桥小脑角病变接受了乙状窦后入路手术,并通过单因素和多因素分析研究了不同因素对脑脊液漏发生的影响。
79例患者(76.7%)因桥小脑角区生长的肿瘤接受手术。24例患者(23.2%)接受微血管减压术治疗耐药性三叉神经痛。16例患者(15.5%)在术后出现脑脊液漏,其中6例接受了手术修复。作为手术操作进行颅骨切除术(P = 0.0450)和进行再次手术(二次手术;P = 0.0079)与发生脑脊液漏的较高风险显著相关。此外,在多因素分析中,进行再次手术成为脑脊液漏发生的独立因素(P = 0.0156)。
接受颅骨切除术的患者和接受二次手术的患者脑脊液漏发生率较高。生物材料技术的不断改进可能有助于神经外科医生预防这种潜在的危及生命的并发症。