From the Department of Diagnostic and Interventional Radiology, Translational Lung Research Center (TLRC), Subdivision of Pulmonary Imaging, University Hospital of Heidelberg, Im Neuenheimer Feld 420, 69120 Heidelberg, Germany (A.B., O.W., R.R., H.U.K., C.P.H., M.O.W.); Translational Lung Research Center Heidelberg (TLRC), German Center for Lung Research (DZL), Heidelberg, Germany (A.B., O.W., R.R., H.U.K., F.T., C.P.H., F.J.F.H., M.O.W.); Department of Diagnostic and Interventional Radiology with Nuclear Medicine (A.B., O.W., R.R., H.U.K., C.P.H., M.O.W.) and Department of Pulmonary Medicine (F.T., F.J.F.H.), Thoraxklinik at the University Hospital of Heidelberg, Heidelberg, Germany; Department of Radiology, Division of Pediatric Radiology, Medical University of Graz, Graz, Austria (A.D.); Department of Internal Medicine II, Division of Pulmonology, Medical University of Vienna, Vienna, Austria (D.G.); Department of Pneumology and Critical Care Medicine, Asklepios Klinik Barmbek, Hamburg, Germany (R.E.); and Institute of Medical Informatics, University of Lübeck, Lübeck, Germany (M.H., F.F.).
Radiol Cardiothorac Imaging. 2024 Oct;6(5):e240041. doi: 10.1148/ryct.240041.
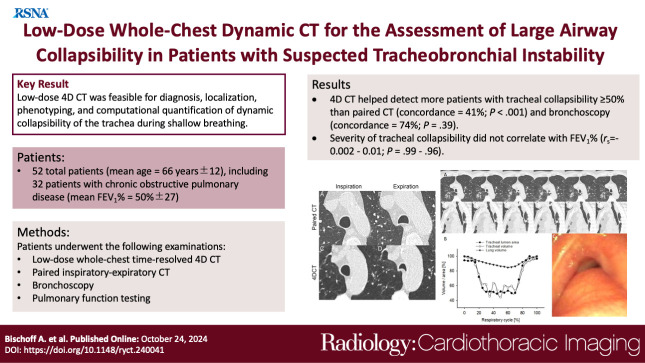
Purpose To quantify tracheal collapsibility using low-dose four-dimensional (4D) CT and to compare visual and quantitative 4D CT-based assessments with assessments from paired inspiratory-expiratory CT, bronchoscopy, and spirometry. Materials and Methods The authors retrospectively analyzed 4D CT examinations (January 2016-December 2022) during shallow respiration in 52 patients (mean age, 66 years ± 12 [SD]; 27 female, 25 male), including 32 patients with chronic obstructive pulmonary disease (mean forced expiratory volume in 1 second percentage predicted [FEV%], 50% ± 27), with suspected tracheal collapse. Paired CT data were available for 27 patients and bronchoscopy data for 46 patients. Images were reviewed by two radiologists in consensus, classifying patients into three groups: 50% or greater tracheal collapsibility, less than 50% collapsibility, or fixed stenosis. Changes in minimal tracheal lumen area, tracheal volume, and lung volume from inspiration to expiration were quantified using YACTA software. Tracheal collapsibility between groups was compared employing one-way analysis of variance (ANOVA). For related samples within one group, ANOVA with repeated measures was used. Spearman rank order correlation coefficient was calculated for collapsibility versus pulmonary function tests. Results At 4D CT, 25 of 52 (48%) patients had tracheal collapsibility of 50% or greater, 20 of 52 (38%) less than 50%, and seven of 52 (13%) had fixed stenosis. Visual assessment of 4D CT detected more patients with collapsibility of 50% or greater than paired CT, and concordance was 41% ( < .001). 4D CT helped identify more patients with tracheal collapsibility of 50% or greater than did bronchoscopy, and concordance was 74% ( = .39). Mean collapsibility of tracheal lumen area and volume at 4D CT were higher for 50% or greater visually assessed collapsibility (area: 53% ± 9 and lumen: 52% ± 10) compared with the less than 50% group (27% ± 9 and 26% ± 6, respectively) ( < .001), whereas both tracheal area and volume were stable for the fixed stenosis group (area: 16% ± 12 and lumen: 21% ± 11). Collapsibility of tracheal lumen area and volume did not correlate with FEV% ( = -0.002 to 0.01, = .99-.96). Conclusion The study demonstrated that 4D CT is feasible and potentially more sensitive than paired CT for central airway collapse. Expectedly, FEV% was not correlated with severity of tracheal collapsibility. CT-Quantitative, Tracheobronchial Tree, Chronic Obstructive Pulmonary Disease, Imaging Postprocessing, Thorax © RSNA, 2024.
目的 使用低剂量四维(4D)CT 定量评估气管塌陷,并比较视觉和基于定量 4D CT 的评估与配对吸气-呼气 CT、支气管镜检查和肺功能检查的评估结果。
材料与方法 本研究回顾性分析了 52 例(平均年龄,66 岁±12[标准差];27 例女性,25 例男性)浅呼吸期间的 4D CT 检查(2016 年 1 月至 2022 年 12 月),这些患者均疑似存在气管塌陷,且均患有慢性阻塞性肺疾病(平均用力呼气量占预计值百分比[FEV%],50%±27)。27 例患者有配对 CT 数据,46 例患者有支气管镜数据。由两位放射科医生共同进行图像评估,将患者分为三组:气管塌陷率≥50%、<50%和固定狭窄。使用 YACTA 软件定量评估最小气管腔面积、气管体积和肺体积在吸气到呼气过程中的变化。采用单因素方差分析(ANOVA)比较各组之间的气管塌陷率。对于同一组内的相关样本,采用重复测量的 ANOVA。计算气管塌陷率与肺功能检查结果之间的 Spearman 秩相关系数。
结果 在 4D CT 上,52 例患者中有 25 例(48%)气管塌陷率≥50%,20 例(38%)<50%,7 例(13%)为固定狭窄。与配对 CT 相比,4D CT 对气管塌陷的视觉评估发现更多的患者存在气管塌陷率≥50%,且一致性为 41%(<.001)。与支气管镜检查相比,4D CT 发现更多的患者存在气管塌陷率≥50%,且一致性为 74%( =.39)。与气管塌陷率<50%的患者相比(面积:27%±9 和管腔:26%±6),视觉评估为气管塌陷率≥50%的患者 4D CT 测量的气管腔面积和体积的平均塌陷率更高(面积:53%±9 和管腔:52%±10)(<.001),而固定狭窄组的气管面积和体积均保持稳定(面积:16%±12 和管腔:21%±11)。气管腔面积和体积的塌陷率与 FEV%无相关性( = -0.002 至 0.01, =.99-.96)。
结论 该研究表明,4D CT 是一种可行的方法,与配对 CT 相比,其对中央气道塌陷的敏感性更高。预期 FEV%与气管塌陷严重程度无相关性。