Cardiovascular Epidemiology Research Centre, School of Population and Global Health, The University of Western Australia, Perth, Western Australia, Australia
Victor Chang Cardiac Research Institute, The University of Western Australia, Perth, Western Australia, Australia.
Open Heart. 2024 Oct 23;11(2):e002995. doi: 10.1136/openhrt-2024-002995.
Since 2000, the definition of myocardial infarction (MI) has evolved with reliance on cardiac troponin (cTn) tests. The implications of this change on trends of acute coronary syndrome (ACS) subtypes obtained from routinely collected hospital morbidity data are unclear. Using person-linked hospitalisation data, we compared International Classification of Diseases (ICD)-coded data with biomarker-classified admission rates for ST-segment elevation MI (STEMI), non-STEMI (NSTEMI) and unstable angina (UA) in Western Australia (WA).
We used linked hospitalisation data from all WA tertiary hospitals to identify patients with a principal diagnosis of STEMI, NSTEMI or UA between 2002 and 2016. Linked biomarker results were classified as 'diagnostic' for MI according to established criteria. We calculated age-standardised and sex-standardised rates (ASSRs) for ICD-coded versus biomarker-classified admissions by ACS subtypes and estimated annual change in admissions using Poisson regression adjusting for age and sex.
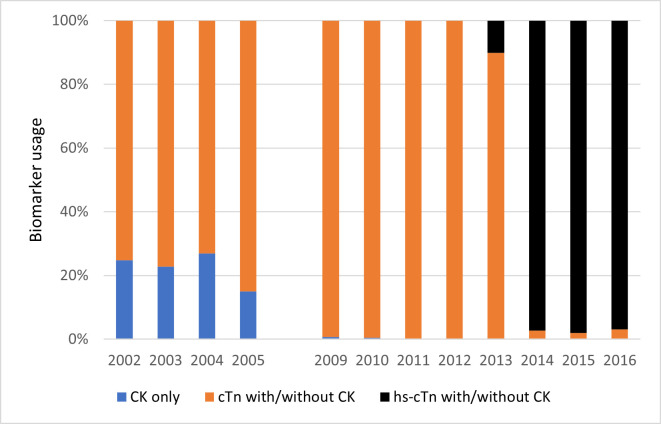
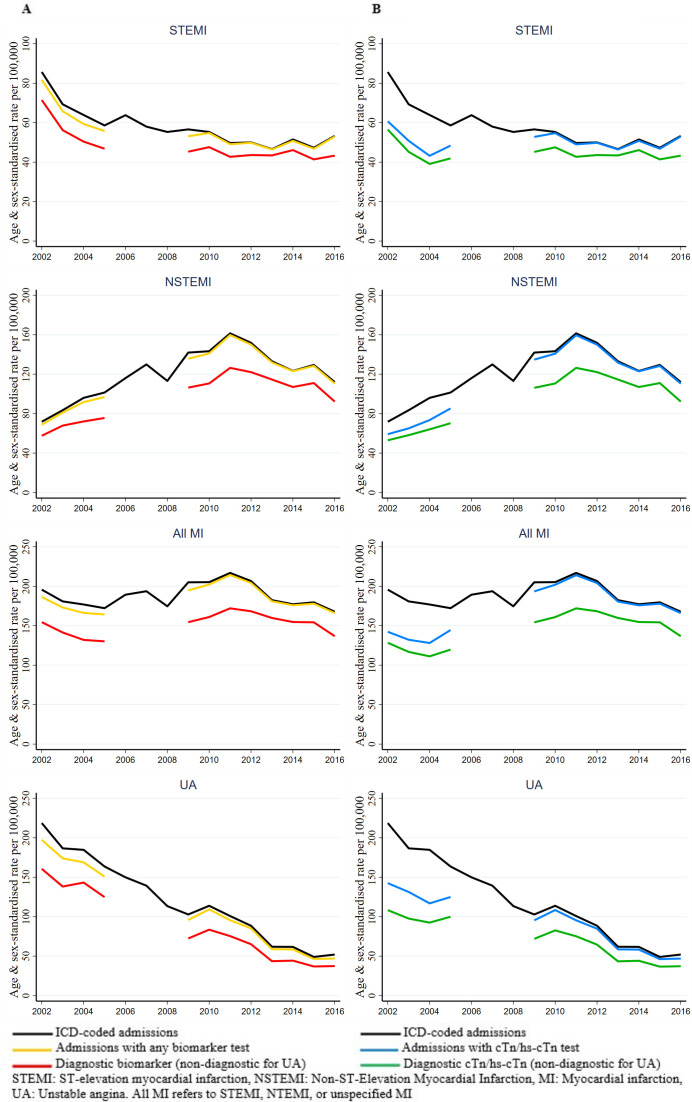
There were 37 272 ACS admissions in 30 683 patients (64.2% male), and 96% of cases had linked biomarker data, predominantly conventional cTn at the start and high-sensitive cTn from late 2013. Despite lower ASSRs, trends in MI classified with a diagnostic biomarker were concordant with ICD-coded admissions rates for both STEMI and NSTEMI. Between 2002 and 2010, STEMI rates declined by 4.1% (95% CI 5.0%, 3.1%) and 3.4% (95% CI 4.6%, 2.3%) in ICD-coded and biomarker-classified admissions, respectively, and both plateaued thereafter. For NSTEMI between 2002 and 2010, the ICD-coded and biomarker-classified rates increased 8.0% per year (95% CI 7.2%, 8.9%) and 8.0% (95% CI 7.0%, 9.0%), respectively, and both subsequently declined. For UA, both ICD-coded and biomarker-classified UA admission rates declined in a steady and concordant manner between 2002 and 2016.
The present study supports the validity of using administrative data to monitor population trends in ACS subtypes as they appear to generally reflect the redefinition of MI in the troponin era.
自 2000 年以来,心肌梗死 (MI) 的定义已经随着对心脏肌钙蛋白 (cTn) 检测的依赖而演变。这一变化对从常规收集的医院发病率数据中获得的急性冠状动脉综合征 (ACS) 亚型趋势的影响尚不清楚。我们使用人员链接的住院数据,比较了国际疾病分类 (ICD) 编码数据与生物标志物分类的西澳大利亚州 (WA) 的 ST 段抬高型心肌梗死 (STEMI)、非 ST 段抬高型心肌梗死 (NSTEMI) 和不稳定型心绞痛 (UA) 的入院率。
我们使用 WA 所有三级医院的链接住院数据,确定了 2002 年至 2016 年间 STEMI、NSTEMI 或 UA 的主要诊断患者。根据既定标准,将链接的生物标志物结果分类为 MI 的“诊断”。我们按 ACS 亚型计算了 ICD 编码与生物标志物分类入院的年龄标准化和性别标准化率 (ASSR),并使用泊松回归估计了按年龄和性别调整后的年度入院变化。
在 30683 名患者中,有 37272 例 ACS 入院患者(64.2%为男性),96%的患者有链接的生物标志物数据,主要是在开始时使用常规 cTn,从 2013 年底开始使用高敏感 cTn。尽管 ASSR 较低,但具有诊断性生物标志物的 MI 趋势与 STEMI 和 NSTEMI 的 ICD 编码入院率一致。2002 年至 2010 年间,ICD 编码和生物标志物分类入院的 STEMI 发生率分别下降了 4.1%(95%CI 5.0%,3.1%)和 3.4%(95%CI 4.6%,2.3%),此后均趋于平稳。2002 年至 2010 年间,NSTEMI 的 ICD 编码和生物标志物分类入院率分别每年增加 8.0%(95%CI 7.2%,8.9%)和 8.0%(95%CI 7.0%,9.0%),此后均有所下降。对于 UA,2002 年至 2016 年间,ICD 编码和生物标志物分类 UA 入院率以稳定且一致的方式下降。
本研究支持使用行政数据监测 ACS 亚型人群趋势的有效性,因为它们似乎普遍反映了肌钙蛋白时代 MI 的重新定义。