School of Population Health M431, University of Western Australia, 35 Stirling Highway, Crawley 6009 WA, Australia.
BMC Cardiovasc Disord. 2011 Jun 24;11:35. doi: 10.1186/1471-2261-11-35.
Troponins (highly sensitive biomarkers of myocardial damage) increase counts of myocardial infarction (MI) in clinical practice, but their impact on trends in admission rates for MI in National statistics is uncertain.
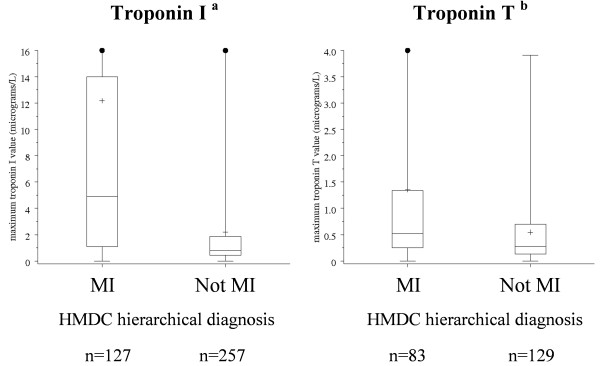
Cases coded as MI or other cardiac diagnoses in the Hospital Morbidity Data Collection (MI-HMDC) in Western Australia in 1998 and 2003 were classified using revised criteria for MI developed by an International panel convened by the American Heart Association (AHA criteria) using information on symptoms, ECGs and cardiac biomarkers abstracted from samples of medical notes. Age-sex standardized rates of MI-HMDC were compared with rates of MI based on AHA criteria including troponins (MI-AHA) or traditional biomarkers only (MI-AHAck).
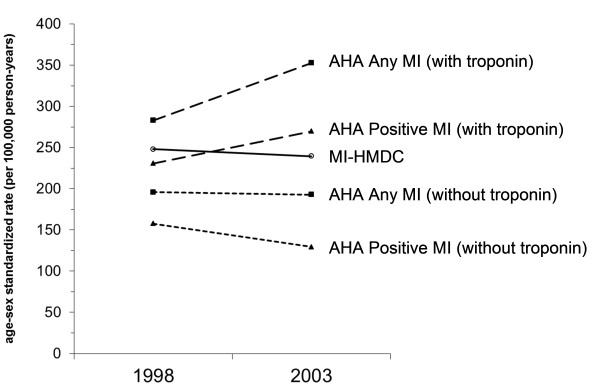
Between 1998 and 2003, rates of MI-HMDC decreased by 3.5% whereas rates of MI-AHA increased by 17%, a difference largely due to increased false-negative cases in the HMDC associated with marked increased use of troponin tests in cardiac admissions generally, and progressively lower test thresholds. In contrast, rates of MI-AHAck declined by 18%.
Increasing misclassification of MI-AHA by the HMDC may be due to reluctance by clinicians to diagnose MI based on relatively small increases in troponin levels. These influences are likely to continue. Monitoring MI using AHA criteria will require calibration of commercially available troponin tests and agreement on lower diagnostic thresholds for epidemiological studies. Declining rates of MI-AHA ck are consistent with long-standing trends in MI in Western Australia, suggesting that neither MI-HMDC nor MI-AHA reflect the true underlying population trends in MI.
肌钙蛋白(心肌损伤的高度敏感生物标志物)在临床实践中增加了心肌梗死(MI)的病例数,但它们对国家统计数据中 MI 入院率趋势的影响尚不确定。
1998 年和 2003 年在西澳大利亚州医院发病率数据收集(MI-HMDC)中编码为 MI 或其他心脏诊断的病例,使用美国心脏协会(AHA)召集的国际小组制定的 MI 修订标准进行分类,这些标准使用从医疗记录样本中提取的症状、心电图和心脏生物标志物信息。MI-HMDC 的年龄性别标准化发病率与基于 AHA 标准的 MI 发病率进行比较,包括肌钙蛋白(MI-AHA)或仅传统生物标志物(MI-AHAck)。
1998 年至 2003 年间,MI-HMDC 的发病率下降了 3.5%,而 MI-AHA 的发病率上升了 17%,这主要是由于 HMDC 中与普遍使用肌钙蛋白检测导致的假阴性病例增加,以及检测阈值逐渐降低有关。相比之下,MI-AHAck 的发病率下降了 18%。
HMDC 对 MI-AHA 的误诊率增加可能是由于临床医生不愿意根据肌钙蛋白水平的相对较小增加来诊断 MI。这些影响可能会持续存在。使用 AHA 标准监测 MI 需要对商业上可用的肌钙蛋白检测进行校准,并就较低的诊断阈值达成共识,以用于流行病学研究。MI-AHAck 发病率的下降与西澳大利亚州 MI 的长期趋势一致,表明 MI-HMDC 和 MI-AHA 均不能反映 MI 的真实人群趋势。