Department of Thoracic and Cardiovascular Surgery, The University of Texas MD Anderson Cancer Center, Houston, Texas, USA.
Department of Biostatistics, The University of Texas MD Anderson Cancer Center, Houston, Texas, USA.
J Immunother Cancer. 2024 Oct 23;12(10):e009677. doi: 10.1136/jitc-2024-009677.
Neoadjuvant immune checkpoint inhibitors (ICIs) have improved survival outcomes compared with chemotherapy in resectable non-small cell lung cancer (NSCLC). However, the impact of actionable genomic alterations (AGAs) on the efficacy of neoadjuvant ICIs remains unclear. We report the influence of AGAs on treatment failure (TF) in patients with resectable NSCLC treated with neoadjuvant ICIs.
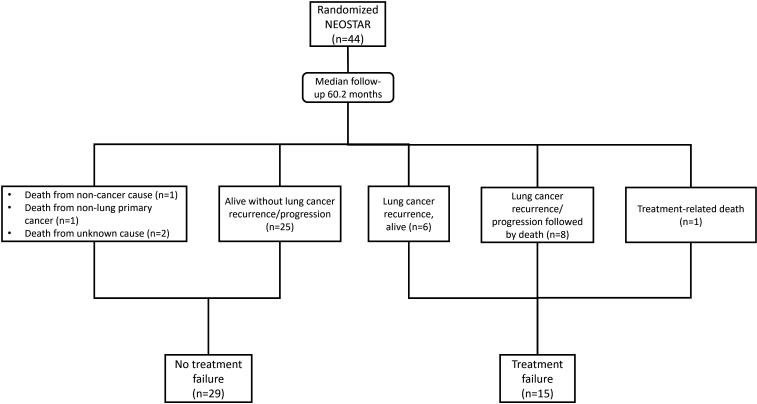
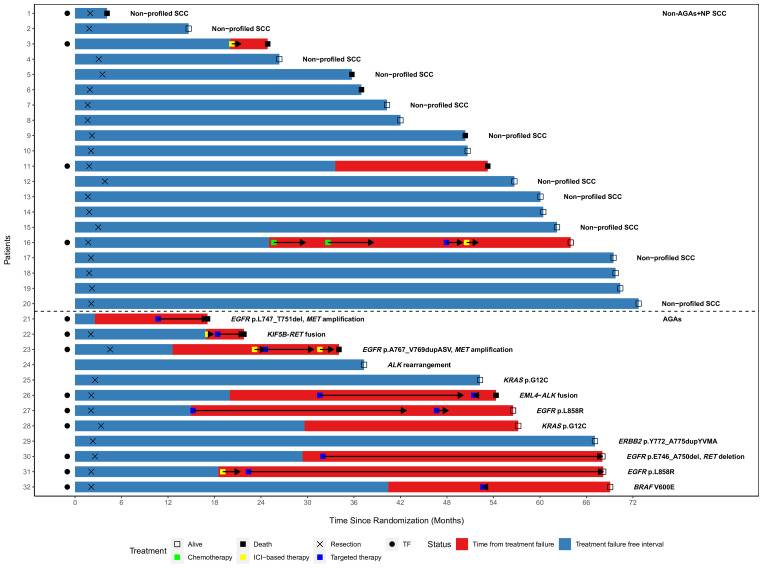
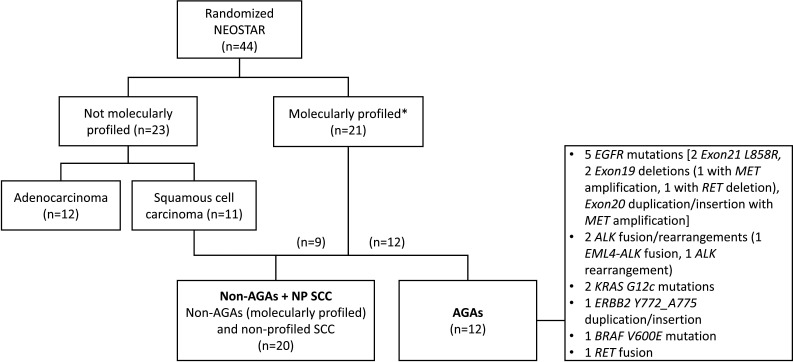
Tumor molecular profiles were obtained from patients with stage I-IIIA resectable NSCLC (American Joint Committee on Cancer seventh edition) treated with either neoadjuvant nivolumab (N, n=23) or nivolumab+ipilimumab (NI, n=21) followed by surgery in a previously reported phase-2 randomized study (NCT03158129). TF was defined as any progression of primary lung cancer after neoadjuvant ICI therapy in patients without surgery, radiographic and/or biopsy-proven primary lung cancer recurrence after surgery, or death from possibly treatment-related complications or from primary lung cancer since randomization. Tumors with AGAs (n=12) were compared with tumors without AGAs and non-profiled squamous cell carcinomas (non-AGAs+NP SCC, n=20).
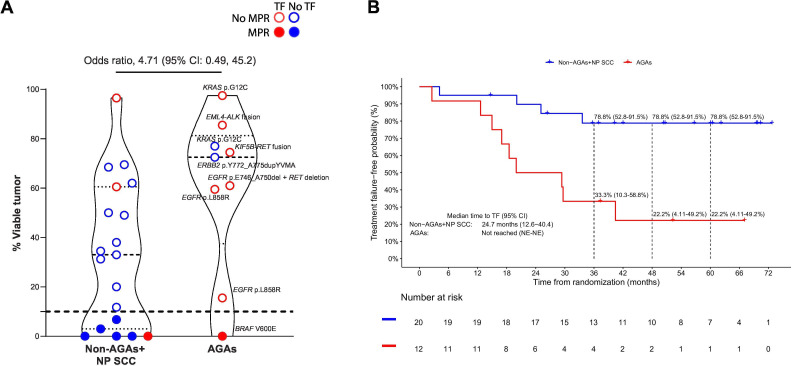
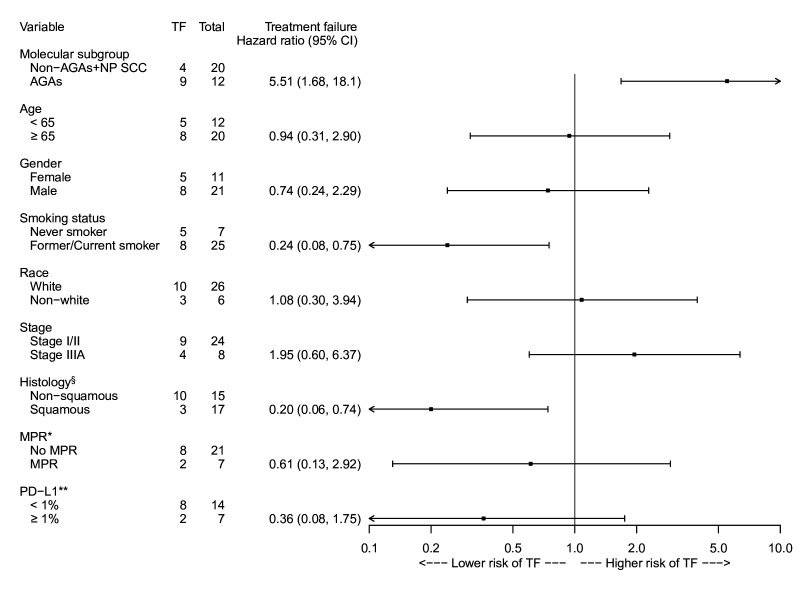
With a median follow-up of 60.2 months, the overall TF rate was 34.1% (15/44). Tumor molecular profiling was retrospectively obtained in 47.7% (21/44) of patients and select AGAs were identified in 12 patients: 5 epidermal growth factor receptor , 2 , 1 , and 1 mutations, 2 anaplastic lymphoma kinase and 1 fusions. The median time to TF in patients with AGAs was 24.7 months (95% CI: 12.6 to 40.4), compared with not reached (95% CI: not evaluable (NE)-NE) in the non-AGAs+NP SCC group. The TF risk was higher in AGAs (HR: 5.51, 95% CI: 1.68 to 18.1), and lower in former/current smokers (HR: 0.24, 95% CI: 0.08 to 0.75). The odds of major pathological response were 4.71 (95% CI: 0.49 to 45.2) times higher in the non-AGAs+NP SCC group, and the median percentage of residual viable tumor was 72.5% in AGAs compared with 33.0% in non-AGS+NP SCC tumors.
Patients with NSCLC harboring select AGAs, including and alterations, have a higher risk for TF, shorter median time to TF, and diminished pathological regression after neoadjuvant ICIs. The suboptimal efficacy of neoadjuvant chemotherapy-sparing, ICI-based regimens in this patient subset underscores the importance of tumor molecular testing prior to initiation of neoadjuvant ICI therapy in patients with resectable NSCLC.
与化疗相比,新辅助免疫检查点抑制剂(ICI)可改善可切除非小细胞肺癌(NSCLC)患者的生存结局。然而,可操作的基因组改变(AGAs)对新辅助 ICI 疗效的影响仍不清楚。我们报告了 AGAs 对接受新辅助 ICI 治疗的可切除 NSCLC 患者治疗失败(TF)的影响。
从接受新辅助纳武单抗(N,n=23)或纳武单抗+伊匹单抗(NI,n=21)治疗的 I 期-IIIA 可切除 NSCLC(美国癌症联合委员会第七版)患者中获得肿瘤分子谱,随后进行手术在以前报道的 2 期随机研究(NCT03158129)中。TF 定义为新辅助 ICI 治疗后原发性肺癌无手术进展,手术后影像学和/或活检证实原发性肺癌复发,或自随机分组以来因可能与治疗相关的并发症或原发性肺癌而死亡的患者的原发性肺癌。将具有 AGAs(n=12)的肿瘤与无 AGAs 和未行分子检测的鳞癌(非 AGAs+NP SCC,n=20)进行比较。
中位随访 60.2 个月,总 TF 率为 34.1%(15/44)。47.7%(44 例中有 21 例)的患者进行了肿瘤分子谱检测,并在 12 例患者中发现了选择性 AGAs:5 例表皮生长因子受体突变,2 例,1 例和 1 例融合,2 例间变性淋巴瘤激酶和 1 例融合。AGAs 组的 TF 中位时间为 24.7 个月(95%CI:12.6 至 40.4),而非 AGAs+NP SCC 组未达到(95%CI:无法评估(NE)-NE)。AGAs 组 TF 风险较高(HR:5.51,95%CI:1.68 至 18.1),前/现吸烟者较低(HR:0.24,95%CI:0.08 至 0.75)。非 AGAs+NP SCC 组主要病理缓解的可能性高 4.71 倍(95%CI:0.49 至 45.2),AGAs 组残留活肿瘤的中位数百分比为 72.5%,而非 AGAs+NP SCC 肿瘤为 33.0%。
携带选择性 AGAs 的 NSCLC 患者,包括 和 改变,TF 风险较高,TF 中位时间较短,新辅助 ICI 后病理缓解程度降低。新辅助化疗节省、基于 ICI 的方案在这部分患者中的疗效不佳,突出了在开始新辅助 ICI 治疗前对可切除 NSCLC 患者进行肿瘤分子检测的重要性。