Zaher Elie, Blumenthal Yonatan, Blumenthal Eytan Z
Department of Ophthalmology, Rambam Health Care Campus, P.O.B 9602, Haifa, 31096, Israel.
Ruth and Bruce Rappaport Faculty of Medicine, Technion - Israel Institute of Technology, Haifa, Israel.
Int J Retina Vitreous. 2024 Oct 24;10(1):80. doi: 10.1186/s40942-024-00601-0.
To present a novel optical model explaining why the vast majority of patients with Asteroid Hyalosis (AH) do not perceive any floaters. This changes our understanding of floater perception and undermines the operation mode of YAG laser vitreolysis.
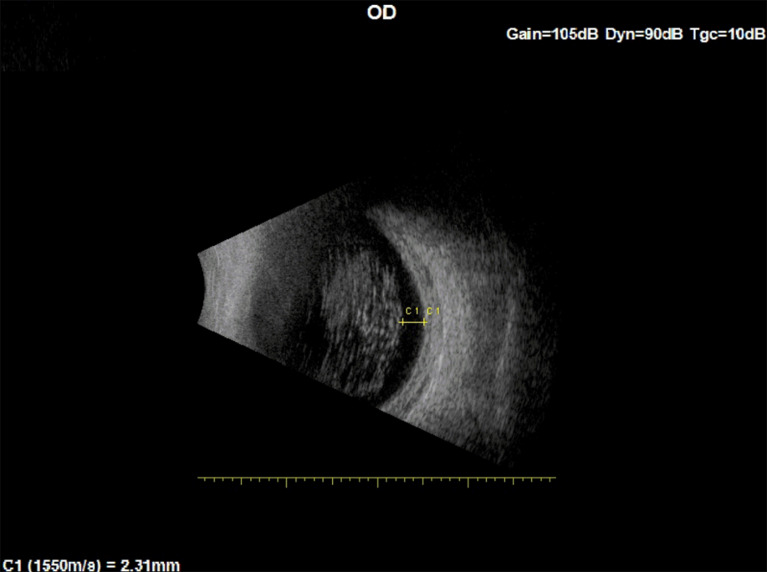
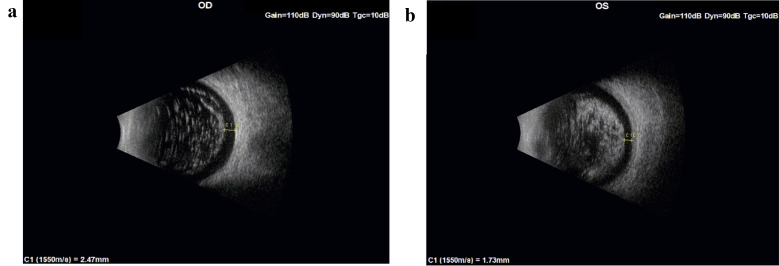
Relying on a previously published model of floater perception based on astronomical equations of a solar eclipse, and on ultrasound images of the vitreous in three eyes with AH, we explain why such patients do not perceive floaters in spite of opaque bodies filling their entire vitreous, to the point of, in severe cases of AH, obscuring the fundus view during ophthalmoscopy.
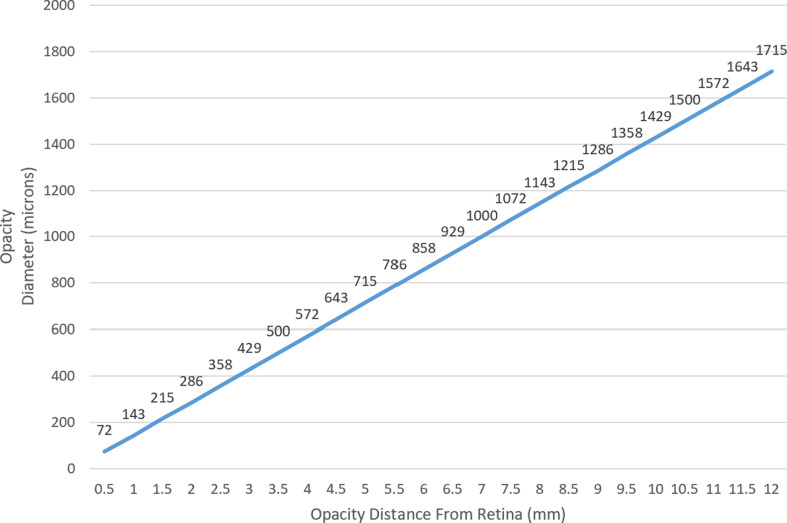
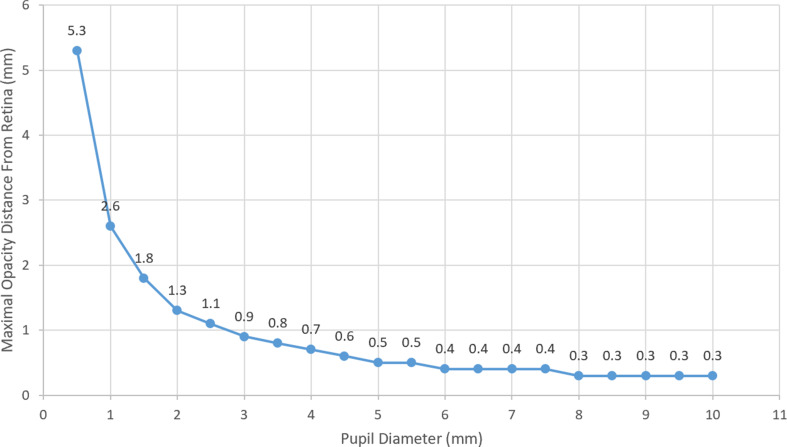
Developing an optical model of light rays that can quantify the maximal distance upon which a vitreous floater or opacity will cast a shadow on the retina.
Calculations using the proposed model demonstrated that with a 3 mm pupil, for a floater located between 1.5 mm and 2 mm from the retina, its shortest diameter must be > 215 microns and > 286 microns, respectively, to be perceived. Since AH floaters, based on ultrasound imaging, do not exist in the most peripheral 1.5 mm of the vitreous, it becomes understandable why these patients are asymptomatic.
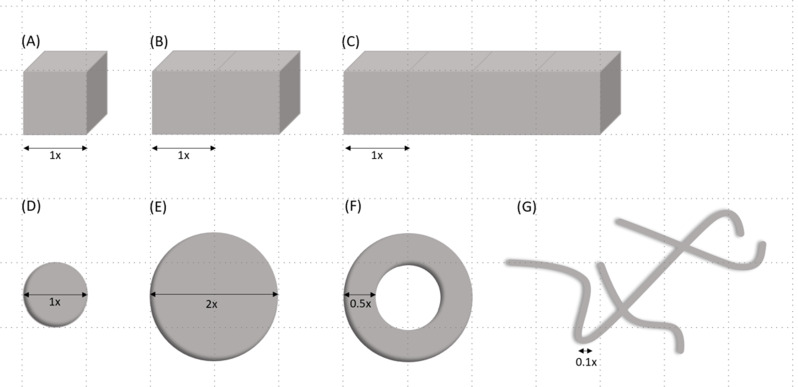
Based on the proposed model and our findings, we deduced that even large, degenerative floaters whose width is usually narrower than a large retinal vein (125 microns), must be located very close to the retina and hence are not the floaters that are aimed at when performing YAG laser vitreolysis. We speculate that in successful cases, YAG vitreolysis works by a different mechanism, most likely a shock wave that displaces floaters further away from the retina. Hence, vitreolysis might not necessarily require the laser be aimed at the floaters, as symptomatic floaters may be located in the outer 1.5-2.0 mm of the vitreous body, a very risky zone for YAG laser shots.
提出一种新颖的光学模型,解释为何绝大多数星状玻璃体变性(AH)患者未察觉到任何飞蚊症。这改变了我们对飞蚊症感知的理解,并对YAG激光玻璃体溶解术的操作模式提出质疑。
基于先前发表的基于日食天文方程的飞蚊症感知模型,以及三只患有AH的眼睛的玻璃体超声图像,我们解释了为何尽管这些患者的整个玻璃体中充满了不透明体,甚至在AH的严重病例中,眼底镜检查时眼底视野被遮挡,但他们仍未察觉到飞蚊症。
建立一个光线光学模型,该模型可以量化玻璃体飞蚊症或混浊物在视网膜上投射阴影的最大距离。
使用所提出的模型进行计算表明,在瞳孔为3毫米的情况下,对于位于距视网膜1.5毫米至2毫米之间的飞蚊症,其最短直径分别必须大于215微米和286微米才能被感知到。根据超声成像,由于AH飞蚊症不存在于玻璃体最周边的1.5毫米范围内,因此这些患者无症状就变得可以理解了。
基于所提出的模型和我们的研究结果,我们推断,即使是通常比粗大视网膜静脉(125微米)窄的大的、退行性飞蚊症,也必须非常靠近视网膜,因此不是进行YAG激光玻璃体溶解术时所针对的飞蚊症。我们推测,在成功的病例中,YAG玻璃体溶解术通过不同的机制起作用,很可能是一种冲击波,将飞蚊症从视网膜上进一步推开。因此,玻璃体溶解术不一定需要将激光对准飞蚊症,因为有症状的飞蚊症可能位于玻璃体的外1.5 - 2.0毫米处,这是YAG激光照射的一个非常危险的区域。