Division of Experimental Medicine, Faculty of Medicine and Health Sciences, McGill University, Montréal, Québec, Canada.
Canadian Medication Appropriateness and Deprescribing Network, Montréal, Québec, Canada.
BMC Infect Dis. 2024 Oct 25;24(1):1204. doi: 10.1186/s12879-024-10105-9.
Older people with HIV (PWH) are at risk of polypharmacy (taking multiple medications). Most medications may be necessary and indicated to manage HIV (e.g., antiretroviral therapy [ART]) and HIV-associated comorbidities. However, some are potentially inappropriate medications (PIMs), defined as causing greater harm than benefit, which leads to medication overload. The objective of this study was to characterize polypharmacy (taking multiple medications) and medication overload (prescription of ≥ 1 PIMs) among older PWH.
This retrospective study included older PWH (aged ≥ 50 years old) attending the tertiary care HIV clinic at the McGill University Health Centre (Montreal, Canada), from June 2022-June 2023. Patient characteristics, medications, and select laboratory values (e.g., CD4 count, hemoglobin A1C) were entered into the MedSafer software identifying PIMs and classifying them according to risk of adverse drug event. We measured the prevalence of polypharmacy (≥ 5 medications prescribed, both including and excluding ART) and medication overload (≥ 1 PIMs). Multivariable logistic regression identified factors associated with medication overload.
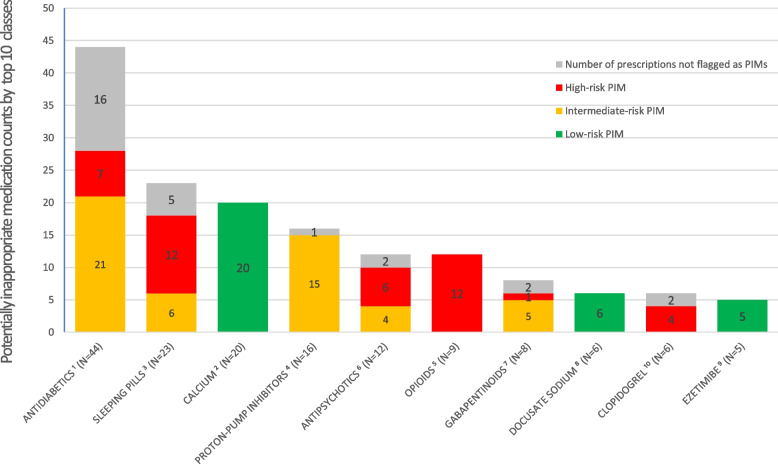
The study included 100 patients, with a median age of 59 years (IQR = 54-63; range 50-82); 42% female. Polypharmacy affected 89% of patients when including antiretroviral therapy (ART) and 60% when excluding ART. Medication overload was present in 58% of patients, and 37.4% of identified PIMs were classified as high-risk. Polypharmacy was the sole predictor of medication overload.
Older PWH are at significant risk of medication overload and receiving higher risk PIMs. Deprescribing PIMs in this population could improve medication appropriateness while reducing the risk of ADEs.
感染艾滋病病毒(HIV)的老年人(PWH)面临着多种药物治疗(服用多种药物)的风险。大多数药物可能是必要的,并被用于治疗 HIV(例如抗逆转录病毒疗法 [ART])和 HIV 相关的合并症。然而,有些药物可能是不适当的(PIMs),定义为弊大于利,从而导致药物过载。本研究的目的是描述老年 PWH 的多种药物治疗(服用多种药物)和药物过载(处方≥1 种 PIMs)的情况。
本回顾性研究纳入了 2022 年 6 月至 2023 年 6 月期间在加拿大麦吉尔大学健康中心(蒙特利尔)三级保健艾滋病毒诊所就诊的老年 PWH(年龄≥50 岁)。患者的特征、药物和一些实验室值(如 CD4 计数、糖化血红蛋白)被输入 MedSafer 软件,以识别 PIMs,并根据不良药物事件的风险对其进行分类。我们测量了多种药物治疗(处方≥5 种药物,包括和不包括 ART)和药物过载(≥1 种 PIMs)的患病率。多变量逻辑回归确定了与药物过载相关的因素。
研究纳入了 100 名患者,中位年龄为 59 岁(IQR=54-63;范围 50-82);42%为女性。包括抗逆转录病毒疗法(ART)时,89%的患者存在多种药物治疗,不包括 ART 时,60%的患者存在多种药物治疗。58%的患者存在药物过载,37.4%的识别出的 PIMs 被归类为高风险。多种药物治疗是药物过载的唯一预测因素。
老年 PWH 面临着药物过载和使用更高风险 PIMs 的重大风险。在该人群中减少 PIMs 的使用可能会提高药物的适当性,同时降低 ADEs 的风险。