From the Abt Associates Inc, Rockville, Maryland.
J Patient Saf. 2020 Sep;16(3S Suppl 1):S23-S35. doi: 10.1097/PTS.0000000000000747.
Approximately 98% of older Americans are simultaneously taking 5-or more-medications to manage at least 2 chronic conditions. Polypharmacy and the use of potentially inappropriate medications (PIMs) are a concern for older adults because they pose a risk for adverse drug events (ADEs), which are associated with emergency department visits and hospitalizations and are an important patient safety priority. We sought to review the evidence of patient safety practices aimed at reducing preventable ADEs in older adults, specifically (i) deprescribing interventions to reduce polypharmacy and (ii) use of the Screening Tool of Older Persons' Potentially Inappropriate Prescriptions (STOPP) to reduce PIMs.
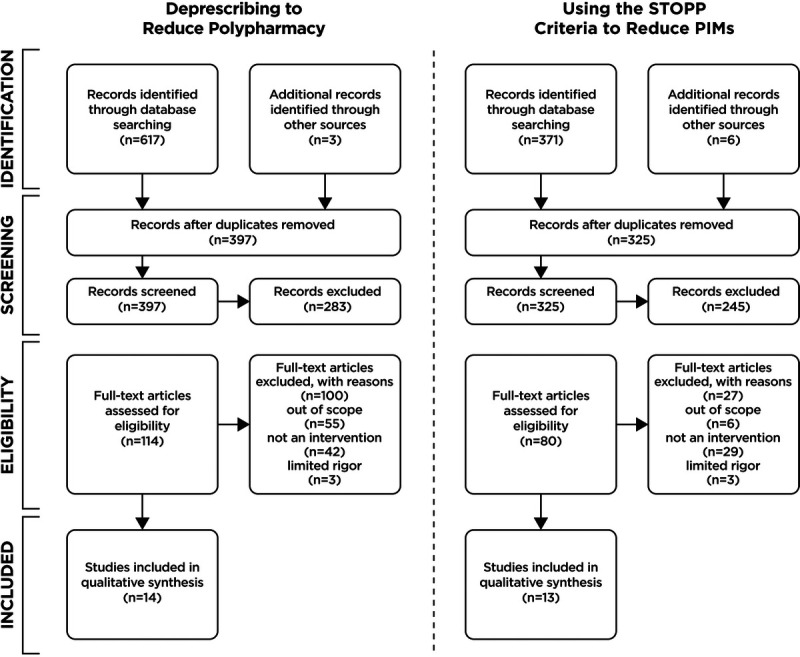
We conducted a systematic review of literature published between 2008 and 2018 that studied examined the effect of these interventions to reduce preventable ADEs in older adults.
Twenty-six studies and 1 systematic review were included (14 for deprescribing and 12 for STOPP and the systematic review). The deprescribing interventions involved decision support tools, educational interventions, and medication reviews by pharmacists and/or providers. Deprescribing studies primarily examined the effect of interventions on process outcomes and observed reductions in polypharmacy, often significantly. A few studies also examined clinical and economic outcomes. Studies of the use of the STOPP screening criteria most commonly reported changes in PIMs, as well as some economic outcomes.
Deprescribing interventions and interventions using the STOPP criteria seem effective in reducing polypharmacy and PIMs in older adults, respectively. Future research on the effectiveness of these approaches on clinical outcomes, the comparative effectiveness of different multicomponent interventions using these approaches, and how to most effectively implement them to improve uptake and evidence-based care is needed.
约 98%的美国老年人同时服用 5 种或更多种药物来治疗至少 2 种慢性病。老年人同时服用多种药物和使用潜在不适当药物(PIMs)令人担忧,因为这会增加药物不良事件(ADEs)的风险,而 ADEs 与急诊就诊和住院有关,是一个重要的患者安全优先事项。我们试图回顾旨在减少老年人可预防 ADEs 的患者安全实践的证据,特别是(i)减少多药治疗的药物停用干预措施,以及(ii)使用老年人潜在不适当处方筛选工具(STOPP)减少 PIMs。
我们对 2008 年至 2018 年间发表的研究文献进行了系统回顾,研究了这些干预措施对减少老年人可预防 ADEs 的效果。
共纳入 26 项研究和 1 项系统评价(14 项关于药物停用,12 项关于 STOPP 和系统评价)。药物停用干预措施涉及决策支持工具、教育干预以及药剂师和/或医务人员进行的药物审查。药物停用研究主要考察了干预措施对过程结果的影响,并观察到多药治疗的减少,通常是显著的。一些研究还考察了临床和经济结果。使用 STOPP 筛选标准的研究最常报告 PIMs 的变化,以及一些经济结果。
药物停用干预措施和使用 STOPP 标准的干预措施分别在减少老年人的多药治疗和 PIMs 方面似乎是有效的。未来需要研究这些方法对临床结果的有效性、使用这些方法的不同多组分干预措施的比较效果,以及如何最有效地实施这些方法以提高采用率和循证护理。