Department of Nephrology, University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK.
Institute of Metabolism and Systems Research, University of Birmingham, Birmingham, UK.
BMC Nephrol. 2024 Oct 25;25(1):379. doi: 10.1186/s12882-024-03763-z.
Patients with diabetes on dialysis experience wide variations in glucose levels and an increased risk of hypoglycaemia. Due to the inaccuracies of HbA1c in dialysis patients, JBDS-IP and KDIGO recommend the use of continuous glucose monitoring (CGM). We conducted a systematic review to examine the current evidence for CGM use and its impact on clinical outcomes in patients with diabetes on dialysis.
A search of MEDLINE(R) ALL, Ovid Emcare, Journals@Ovid Full Text and Embase databases were conducted. Clinical or observational trials in adults with Type 1(T1D) or Type 2 (T2D) diabetes on dialysis and CGM intervention reporting on glycaemic outcomes were included.
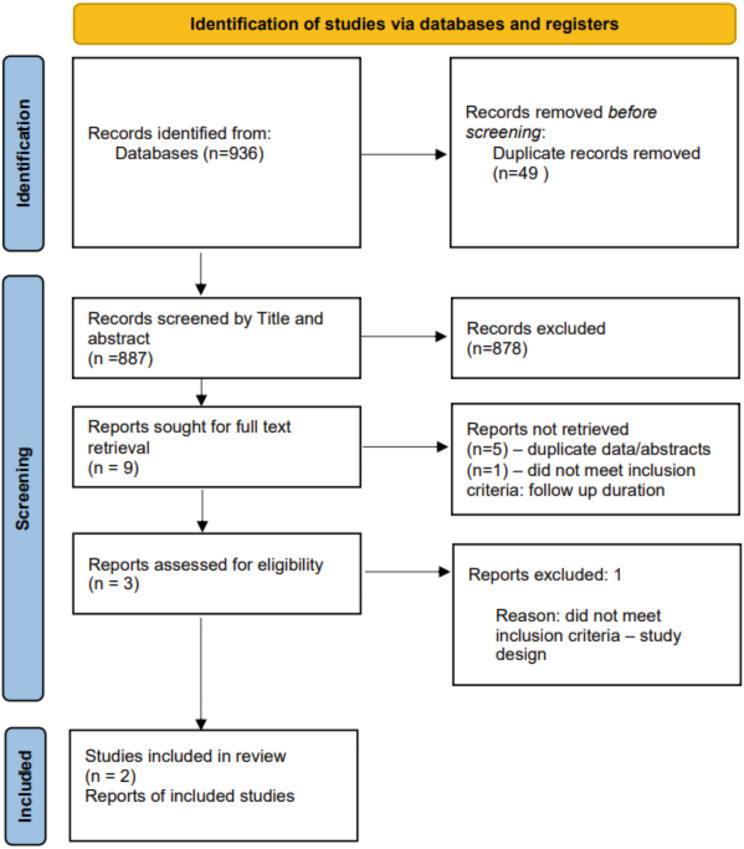
Of the 936 citations identified, 49 duplicates were removed. 887 citations were screened by title and abstract. 9 full texts were reviewed and a further 7 excluded due to duplications or failure to meet to selection criteria. Data was extracted for 2 studies, both prospective before-and-after interventional studies with no control group. Joubert et al. (2015) showed results for 15 participants with T1D. Mean CGM glucose level decreased from 8.37mmol/L at baseline to 7.7mmol/L at the end of the CGM period (p < 0.05) while HbA1c decreased from 6.9 to 6.5% (p < 0.05) during the same period. Mean CGM was lower on dialysis days (7.68mmol/L vs. 7.8mmol/L, p < 0.05). Képénékian et al. (2014) reported on data from 29 T2D patients. Following a 3 month CGM-adapted insulin regimen, HbA1c decreased from 8.4% at baseline to 7.6% (p < 0.01) by the end of study. Mean CGM values decreased from 9.9mmol/L to 8.9mmol/L (p = 0.05) and the frequency of glucose values > 10mmol/L decreased from 41 to 30% (p < 0.05), without a significant increase in hypoglycaemia frequency. Both studies were deemed to be of 'good' quality.
Evidence demonstrating the benefits of CGM in patients with diabetes receiving dialysis is lacking. There is a need for well-designed randomised controlled trials to ascertain the benefits of this technology in this patient group.
PROSPERO registration number: CRD42023371635, https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=371635 .
接受透析治疗的糖尿病患者血糖水平波动较大,且低血糖风险增加。由于 HbA1c 在透析患者中的准确性不足,JBDS-IP 和 KDIGO 建议使用连续血糖监测(CGM)。我们进行了一项系统评价,以评估 CGM 在透析患者中的应用现状及其对临床结局的影响。
检索 MEDLINE(R) ALL、Ovid Emcare、Journals@Ovid Full Text 和 Embase 数据库。纳入成人 1 型(T1D)或 2 型(T2D)糖尿病接受透析和 CGM 干预并报告血糖结局的临床或观察性试验。
在 936 条引文中共发现 49 条重复引文,887 条引文经标题和摘要筛选,9 篇全文进行了回顾,另外 7 篇由于重复或不符合入选标准而被排除。对 2 项研究的数据进行了提取,这两项研究均为前瞻性、干预前后研究,没有对照组。Joubert 等人(2015 年)的研究结果显示了 15 名 T1D 参与者的数据。CGM 平均血糖水平从基线时的 8.37mmol/L 降至 CGM 期结束时的 7.7mmol/L(p<0.05),同时 HbA1c 从 6.9%降至 6.5%(p<0.05)。CGM 在透析日的平均值较低(7.68mmol/L 与 7.8mmol/L,p<0.05)。Képénékian 等人(2014 年)报告了 29 名 T2D 患者的数据。在接受 3 个月 CGM 调整胰岛素治疗后,HbA1c 从基线时的 8.4%降至研究结束时的 7.6%(p<0.01)。CGM 平均血糖值从 9.9mmol/L 降至 8.9mmol/L(p=0.05),血糖值>10mmol/L 的频率从 41%降至 30%(p<0.05),低血糖频率无显著增加。这两项研究均被认为质量较好。
目前缺乏 CGM 在接受透析治疗的糖尿病患者中获益的证据。需要进行精心设计的随机对照试验,以确定该技术在该患者群体中的获益。
PROSPERO 注册号:CRD42023371635,https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=371635 。