Department of Cardiology, Kawaguchi Municipal Medical Center, Kawaguchi 333-0833, Japan.
Department of Cardiology, Nihon University Hospital, Tokyo 101-8309, Japan.
Medicina (Kaunas). 2024 Sep 25;60(10):1575. doi: 10.3390/medicina60101575.
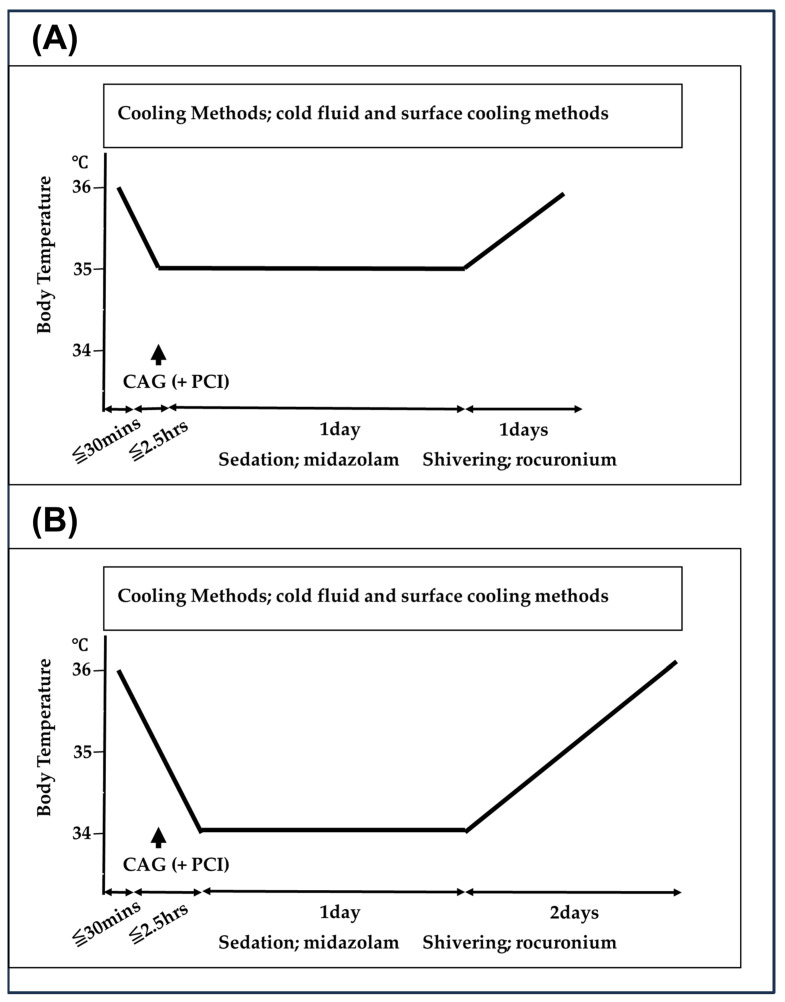
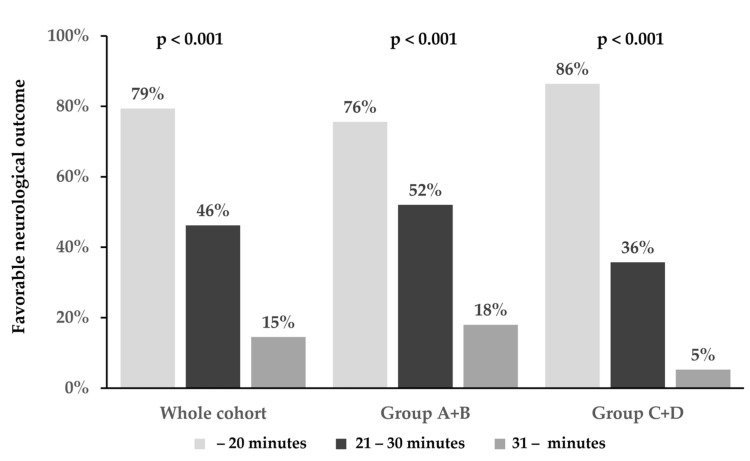
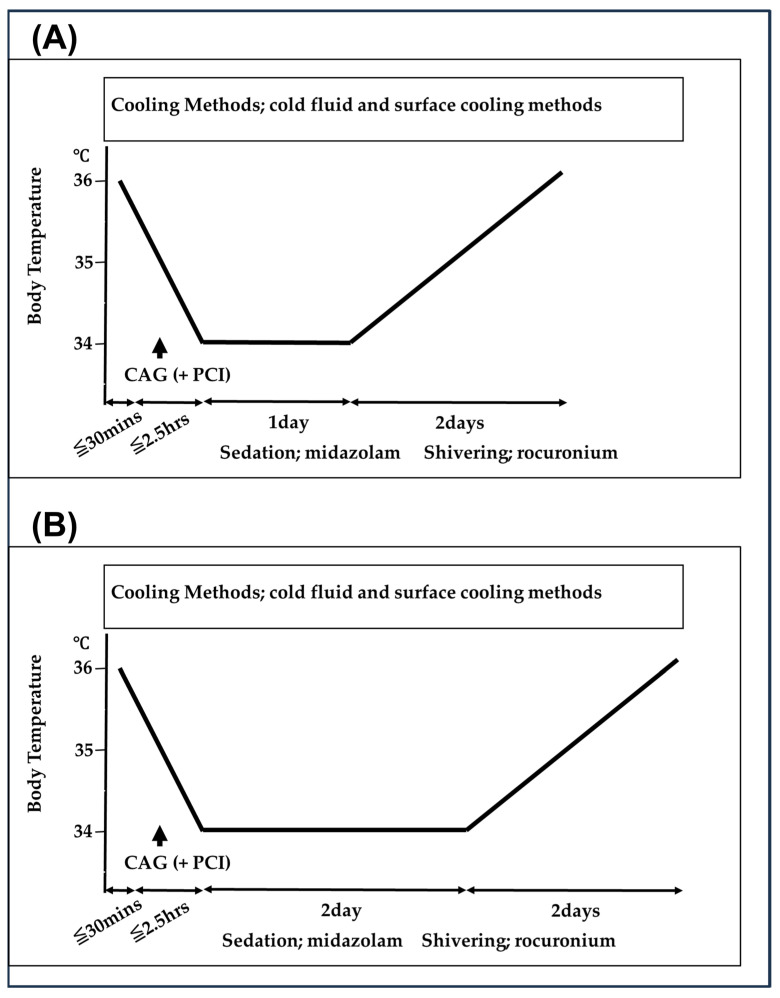
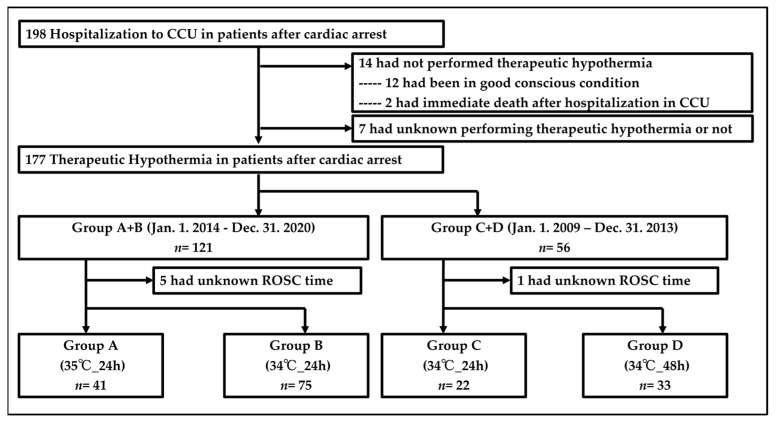
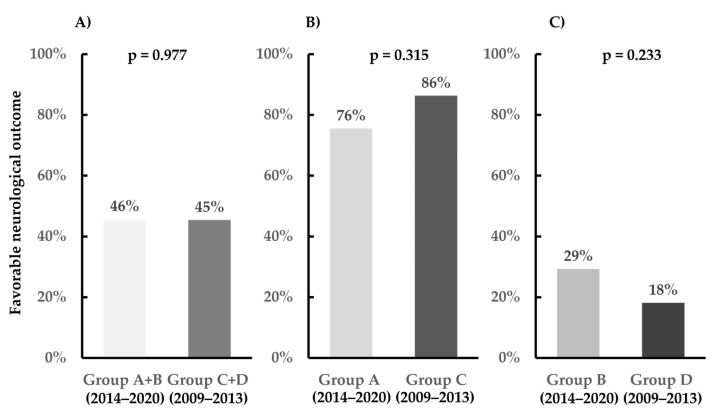
: To prevent hypoxic-ischemic brain damage in patients with post-cardiac arrest syndrome (PCAS), international guidelines have emphasized performing targeted temperature management (TTM). However, the most optimal targeted core temperature and cooling duration reached no consensus to date. This study aimed to clarify the optimal targeted core temperature and cooling duration, selected according to the time interval from collapse to return of spontaneous circulation (ROSC) in patients with PCAS due to cardiac etiology. : Between 2014 and 2020, the targeted core temperature was 34 °C or 35 °C, and the cooling duration was 24 h. If the time interval from collapse to ROSC was within 20 min, we performed the 35 °C targeted core temperature (Group A), and, if not, we performed the 34 °C targeted core temperature (Group B). Between 2009 and 2013, the targeted core temperature was 34 °C, and the cooling duration was 24 or 48 h. If the interval was within 20 min, we performed the 24 h cooling duration (Group C), and, if not, we performed the 48 h cooling duration (Group D). : The favorable neurological outcome rates at 30 days following cardiac arrest were 45.7% and 45.5% in Groups A + B and C + D, respectively ( = 0.977). In patients with ROSC within 20 min, the favorable neurological outcome rates at 30 days following cardiac arrest were 75.6% and 86.4% in Groups A and C, respectively ( = 0.315). In patients with ROSC ≥ 21 min, the favorable neurological outcome rates at 30 days following cardiac arrest were 29.3% and 18.2% in Groups B and D, respectively ( = 0.233). : Selecting the optimal target core temperature and the cooling duration for TTM, according to the time interval from collapse to ROSC, may be helpful in patients with PCAS due to cardiac etiology.
为了预防心搏骤停后综合征(PCAS)患者的缺氧缺血性脑损伤,国际指南强调进行目标温度管理(TTM)。然而,迄今为止,对于最佳的目标核心温度和冷却持续时间尚未达成共识。本研究旨在阐明根据心因性 PCAS 患者从心脏骤停到自主循环恢复(ROSC)的时间间隔选择最佳的目标核心温度和冷却持续时间。
在 2014 年至 2020 年期间,目标核心温度为 34°C 或 35°C,冷却持续时间为 24 小时。如果从心脏骤停到 ROSC 的时间间隔在 20 分钟内,我们将进行 35°C 的目标核心温度(A 组),否则我们将进行 34°C 的目标核心温度(B 组)。在 2009 年至 2013 年期间,目标核心温度为 34°C,冷却持续时间为 24 或 48 小时。如果间隔时间在 20 分钟内,我们将进行 24 小时的冷却持续时间(C 组),否则我们将进行 48 小时的冷却持续时间(D 组)。
心脏骤停后 30 天的神经功能良好结局率在 A + B 组和 C + D 组分别为 45.7%和 45.5%(=0.977)。在 ROSC 发生在 20 分钟内的患者中,心脏骤停后 30 天的神经功能良好结局率在 A 组和 C 组分别为 75.6%和 86.4%(=0.315)。在 ROSC≥21 分钟的患者中,心脏骤停后 30 天的神经功能良好结局率在 B 组和 D 组分别为 29.3%和 18.2%(=0.233)。
根据从心脏骤停到 ROSC 的时间间隔选择 TTM 的最佳目标核心温度和冷却持续时间,可能有助于心因性 PCAS 患者。