Pittsburgh Post-Cardiac Arrest Service, Department of Emergency Medicine, University of Pittsburgh, Pittsburgh, Pennsylvania.
JAMA Netw Open. 2020 Jul 1;3(7):e208215. doi: 10.1001/jamanetworkopen.2020.8215.
It is uncertain what the optimal target temperature is for targeted temperature management (TTM) in patients who are comatose following cardiac arrest.
To examine whether illness severity is associated with changes in the association between target temperature and patient outcome.
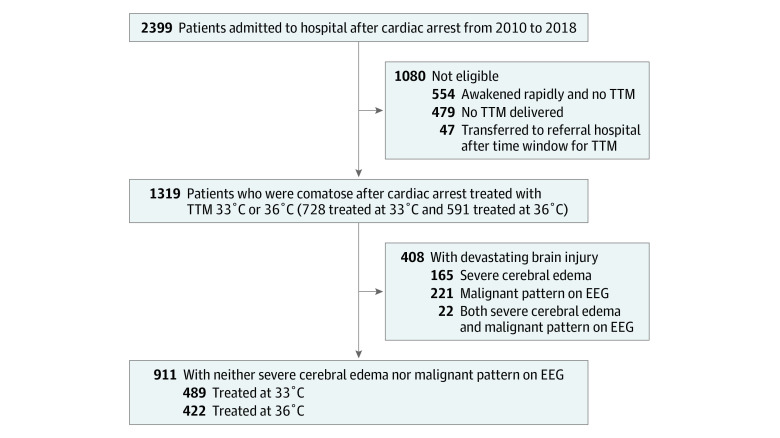
DESIGN, SETTING, AND PARTICIPANTS: This cohort study compared outcomes for 1319 patients who were comatose after cardiac arrest at a single center in Pittsburgh, Pennsylvania, from January 2010 to December 2018. Initial illness severity was based on coma and organ failure scores, presence of severe cerebral edema, and presence of highly malignant electroencephalogram (EEG) after resuscitation.
TTM at 36 °C or 33 °C.
Primary outcome was survival to hospital discharge, and secondary outcomes were modified Rankin Scale and cerebral performance category.
Among 1319 patients, 728 (55.2%) had TTM at 33 °C (451 [62.0%] men; median [interquartile range] age, 61 [50-72] years) and 591 (44.8%) had TTM at 36 °C (353 [59.7%] men; median [interquartile range] age, 59 [48-69] years). Overall, 184 of 187 patients (98.4%) with severe cerebral edema died and 234 of 243 patients (96.3%) with highly malignant EEG died regardless of TTM strategy. Comparing TTM at 33 °C with TTM at 36 °C in 911 patients (69.1%) with neither severe cerebral edema nor highly malignant EEG, survival was lower in patients with mild to moderate coma and no shock (risk difference, -13.8%; 95% CI, -24.4% to -3.2%) but higher in patients with mild to moderate coma and cardiopulmonary failure (risk difference, 21.8%; 95% CI, 5.4% to 38.2%) or with severe coma (risk difference, 9.7%; 95% CI, 4.0% to 15.3%). Interactions were similar for functional outcomes. Most deaths (633 of 968 [65.4%]) resulted after withdrawal of life-sustaining therapies.
In this study, TTM at 33 °C was associated with better survival than TTM at 36 °C among patients with the most severe post-cardiac arrest illness but without severe cerebral edema or malignant EEG. However, TTM at 36 °C was associated with better survival among patients with mild- to moderate-severity illness.
对于心脏骤停后昏迷的患者,目标体温管理(TTM)的最佳目标温度尚不确定。
研究疾病严重程度是否与目标温度与患者预后之间的关联变化有关。
设计、地点和参与者:这项队列研究比较了 2010 年 1 月至 2018 年 12 月在宾夕法尼亚州匹兹堡的一家单一中心因心脏骤停而昏迷的 1319 名患者的结局。初始疾病严重程度基于昏迷和器官衰竭评分、是否存在严重脑水肿以及复苏后是否存在高度恶性脑电图(EEG)。
36°C 或 33°C 的 TTM。
主要结局是出院时的存活,次要结局是改良的兰金量表和脑功能分类。
在 1319 名患者中,728 名(55.2%)接受了 33°C 的 TTM(451 名[62.0%]男性;中位[四分位距]年龄,61[50-72]岁),591 名(44.8%)接受了 36°C 的 TTM(353 名[59.7%]男性;中位[四分位距]年龄,59[48-69]岁)。总体而言,187 名(98.4%)有严重脑水肿的患者和 243 名(96.3%)有高度恶性 EEG 的患者无论 TTM 策略如何,均死亡。在 911 名(69.1%)无严重脑水肿和无高度恶性 EEG 的患者中,与 33°C 的 TTM 相比,36°C 的 TTM 患者中轻度至中度昏迷且无休克的患者存活率较低(风险差异,-13.8%;95%CI,-24.4%至-3.2%),但轻度至中度昏迷和心肺衰竭(风险差异,21.8%;95%CI,5.4%至 38.2%)或严重昏迷(风险差异,9.7%;95%CI,4.0%至 15.3%)患者的存活率较高。功能结局的交互作用相似。大多数死亡(968 例中的 633 例[65.4%])发生在停止维持生命的治疗之后。
在这项研究中,与 36°C 的 TTM 相比,33°C 的 TTM 与心脏骤停后最严重疾病患者的存活率更高,但无严重脑水肿或恶性 EEG。然而,在轻度至中度疾病患者中,36°C 的 TTM 与更好的存活率相关。