Department of Anesthesiology and Reanimation, Lapseki State Hospital, Canakkale, Turkey.
Department of Anesthesiology and Reanimation, Beykent University, Istanbul, Turkey.
Medicine (Baltimore). 2024 Oct 11;103(41):e40053. doi: 10.1097/MD.0000000000040053.
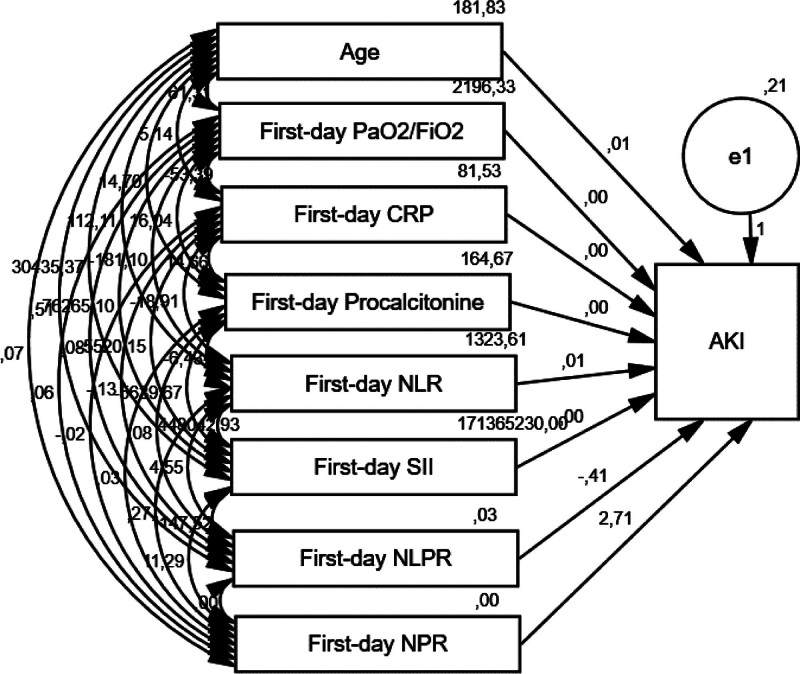
Acute kidney injury (AKI) is one of the most seen complications of coronavirus-2019 (COVID-19) infection. Patients with AKI caused by COVID-19 likely have higher neutrophil counts and lower platelet and lymphocyte levels. Therefore, the predictive value of many inflammation indexes calculated from the total blood count has been investigated to predict the AKI in COVID-19. According to our clinical experience, we thought that neutrophilia and thrombocytopenia may be more common in the development of AKI. For this reason, this study aimed to evaluate the predictive value of the neutrophil-to-platelet ratio (NPR) for AKI in severe COVID-19 patients. This retrospective study included 334 severe COVID-19 patients followed up in the intensive care unit (ICU). Predictive factors for AKI were analyzed. ROC curve analysis was performed to determine the inflammation indexes' cutoff values for the AKI prediction. Multivariate analyses were performed to determine correlations between the inflammation indexes and AKI. In this study, AKI was determined at the rate of 43% (n:145). Independent risk factors affecting AKI were determined to be age (HR = 1.047, 95% confidence interval [CI]: 1.021-1.072, P < .001), the need for invasive mechanical ventilation (HR = 3.003, 95% CI: 1.645-5.481, P = .001) and the need for vasopressor (HR = 8.111, 95% CI: 3.786-17.375, P < .001). The optimal cutoff values predicting AKI were determined to be 3.9 for the NPR (AUC = 0.679, 95% CI: 0.622-0.737, P < .001) with 71.7% sensitivity and 61.9% specificity, 16.1 for the neutrophil-to-lymphocyte ratio (NLR) (AUC = 0.634, 95% CI: 0.575-0.694, P < .001) with 65.5% sensitivity and 56.1% specificity, and 3872.5 × 109L for the systemic inflammatory index (SII) (AUC = 0.566, 95% CI: 0.504-0.629, P = .038) with 60% sensitivity and 55.6% specificity. In the regression model, only NPR values above the cutoff were related to AKI (HR = 3.817, 95% CI: 1.782-8.177, P = .001). The NPR has more predictive value than the NLPR, NLR, and SII in developing AKI in severe COVID-19 patients in the ICU. NPR is a new helpful index that can help clinicians predict early AKI in critical COVID-19.
急性肾损伤(AKI)是 2019 年冠状病毒(COVID-19)感染最常见的并发症之一。由 COVID-19 引起的 AKI 患者的中性粒细胞计数可能较高,血小板和淋巴细胞水平较低。因此,已经研究了许多从全血细胞计算得出的炎症指标的预测值,以预测 COVID-19 中的 AKI。根据我们的临床经验,我们认为中性粒细胞增多和血小板减少可能更常见于 AKI 的发展。出于这个原因,本研究旨在评估中性粒细胞与血小板比值(NPR)对严重 COVID-19 患者 AKI 的预测价值。这项回顾性研究纳入了在重症监护病房(ICU)接受随访的 334 例严重 COVID-19 患者。分析 AKI 的预测因素。进行 ROC 曲线分析以确定炎症指标预测 AKI 的截断值。进行多变量分析以确定炎症指标与 AKI 之间的相关性。在这项研究中,AKI 的发生率为 43%(n:145)。确定影响 AKI 的独立危险因素为年龄(HR=1.047,95%置信区间[CI]:1.021-1.072,P<.001)、需要有创机械通气(HR=3.003,95%CI:1.645-5.481,P=.001)和需要血管加压药(HR=8.111,95%CI:3.786-17.375,P<.001)。预测 AKI 的最佳截断值被确定为 NPR 为 3.9(AUC=0.679,95%CI:0.622-0.737,P<.001),敏感性为 71.7%,特异性为 61.9%,中性粒细胞与淋巴细胞比值(NLR)为 16.1(AUC=0.634,95%CI:0.575-0.694,P<.001),敏感性为 65.5%,特异性为 56.1%,全身炎症指数(SII)为 3872.5×109/L(AUC=0.566,95%CI:0.504-0.629,P=.038),敏感性为 60%,特异性为 55.6%。在回归模型中,只有超过截断值的 NPR 值与 AKI 相关(HR=3.817,95%CI:1.782-8.177,P=.001)。在 ICU 中,NPR 比 NLR、NLR 和 SII 对严重 COVID-19 患者 AKI 的发展具有更高的预测价值。NPR 是一种新的有用指标,可以帮助临床医生预测严重 COVID-19 患者的早期 AKI。