Department of Radiation Oncology, Tohoku University Graduate School of Medicine, Sendai, Japan.
PLoS One. 2024 Oct 30;19(10):e0312032. doi: 10.1371/journal.pone.0312032. eCollection 2024.
This study aimed to investigate the intrafractional movement of the spinal cord and spinal canal during MR-guided online adaptive radiotherapy (MRgART) for kidney cancer.
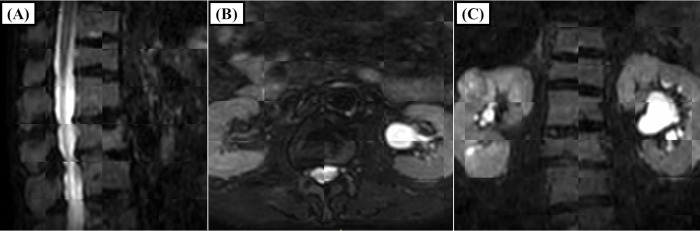
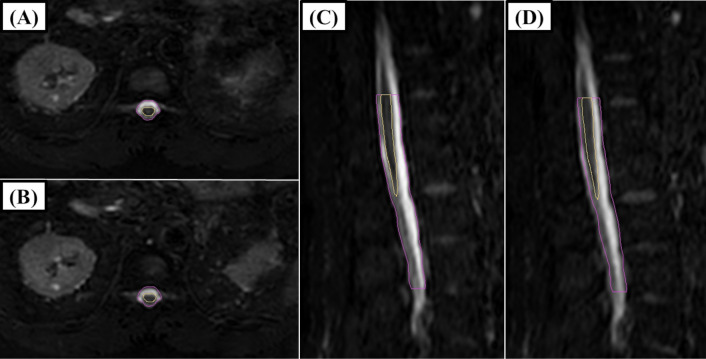
All patients who received stereotactic MRgART for kidney cancer between February 2022 and February 2024 were included in this study. Patients received 30-42 Gy in 3-fraction MRgART for kidney cancer using the Elekta Unity, which is equipped with a linear accelerator and a 1.5 Tesla MRI. MRI scans were performed at three points during each fraction: for online planning, position verification, and posttreatment assessment. The spinal cord was contoured from the upper edge of Th12 to the medullary cone, and the spinal canal was contoured from Th12 to L3, using the first MRI. These contours were adjusted to the second and third MR images via deformable image registration, and movements were measured. Margins were determined via the formula "1.3×Σ+0.5×σ" and 95% prediction intervals.
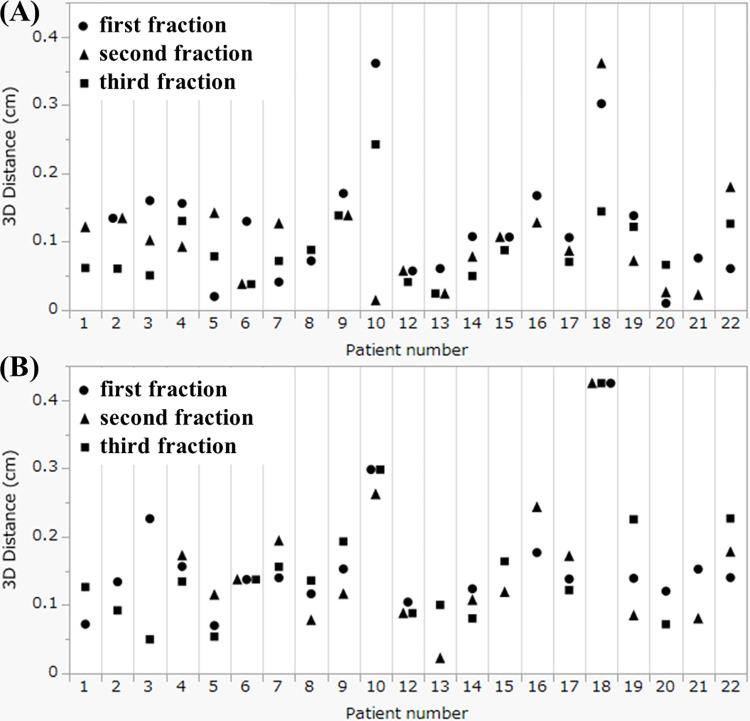
A total of 22 patients (66 fractions) were analyzed. The median interval between the first and third MRI scans were 38 minutes. The mean ± standard deviation of the spinal cord movements after this interval were -0.01 ± 0.06 for the x-axis (right-left), 0.01 ± 0.14 for the y-axis (caudal-cranial), 0.07 ± 0.05 for the z-axis (posterior-anterior), and 0.15 ± 0.08 for the 3D distance, respectively. The correlation coefficients of the 3D distance between the spinal cord and the spinal canal was high (0.92). The calculated planning organ at risk volume margin for all directions was 0.11 cm for spinal cord. The 95% prediction intervals for the x-axis, y-axis, and z-axis were -0.11-0.09 cm, -0.23-0.25 cm and -0.14-0.03 cm, respectively.
Margins are necessary in MRgART to compensate for intrafractional movement and ensure safe treatment delivery.
本研究旨在探讨磁共振引导在线自适应放疗(MRgART)治疗肾癌过程中脊髓和椎管的分次内运动。
本研究纳入了 2022 年 2 月至 2024 年 2 月期间接受立体定向 MRgART 治疗的肾癌患者。患者接受 30-42 Gy 的 3 分次 MRgART 治疗,使用配备直线加速器和 1.5T MRI 的 Elekta Unity。在每分次的三个时间点进行 MRI 扫描:在线计划、位置验证和治疗后评估。使用第一次 MRI 勾画脊髓上界为 Th12,下界为脊髓圆锥,勾画椎管下界为 Th12,上界为 L3。通过变形图像配准将这些轮廓调整至第二和第三次 MRI 图像,并测量运动。边界通过公式“1.3×Σ+0.5×σ”和 95%预测区间确定。
共分析了 22 例患者(66 分次)。第一次和第三次 MRI 扫描之间的中位时间间隔为 38 分钟。间隔后脊髓运动的平均值±标准差分别为 x 轴(左右)-0.01±0.06、y 轴(头尾)0.01±0.14、z 轴(前后)0.07±0.05 和 3D 距离 0.15±0.08。脊髓和椎管的 3D 距离相关系数较高(0.92)。所有方向的计划器官受照体积边界均为 0.11cm。x 轴、y 轴和 z 轴的 95%预测区间分别为-0.11-0.09cm、-0.23-0.25cm 和-0.14-0.03cm。
MRgART 中需要边界来补偿分次内运动,以确保安全的治疗传递。