Nissen Alexander P, Duwayri Yazan M, Jordan William D, Babaliaros Vasilis C, Lederman Robert J, Leshnower Bradley G
Division of Cardiothoracic Surgery, Emory University School of Medicine, Atlanta, Ga.
Division of Vascular Surgery, Emory University School of Medicine, Atlanta, Ga.
JTCVS Tech. 2024 Jul 25;27:19-28. doi: 10.1016/j.xjtc.2024.07.007. eCollection 2024 Oct.
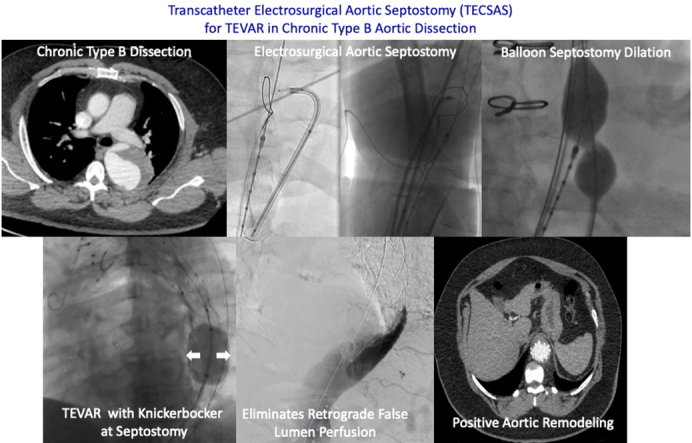
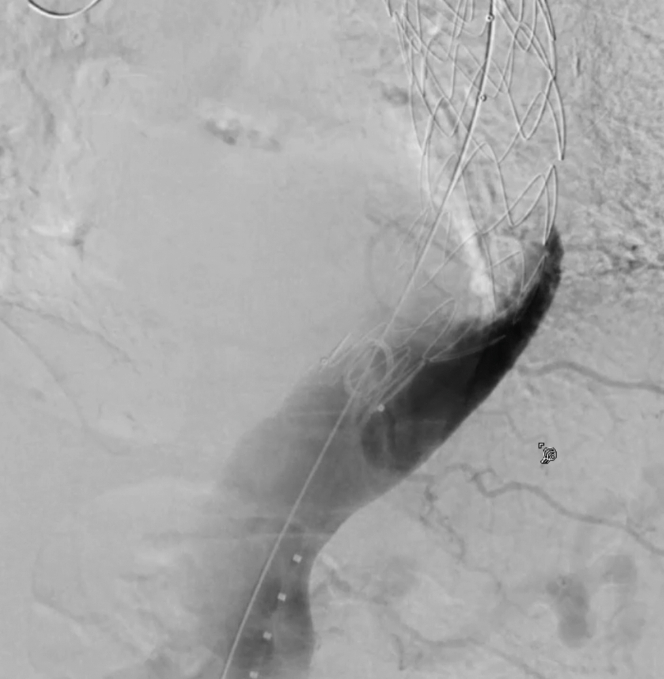
Efficacy of thoracic endovascular aortic repair (TEVAR) for chronic type B aortic dissection (CTBAD) is dependent on eliminating retrograde false lumen perfusion and remodeling the aorta. We describe the efficacy of a novel transcatheter electrosurgical technique to fenestrate the dissection flap and create a distal seal zone for TEVAR in CTBAD.
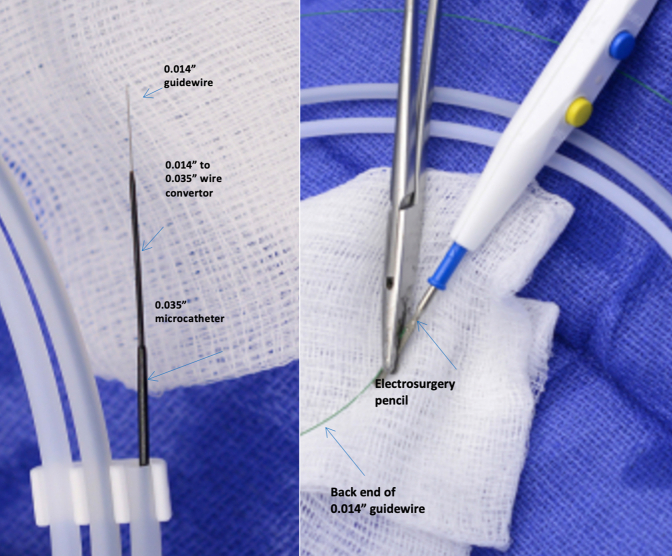
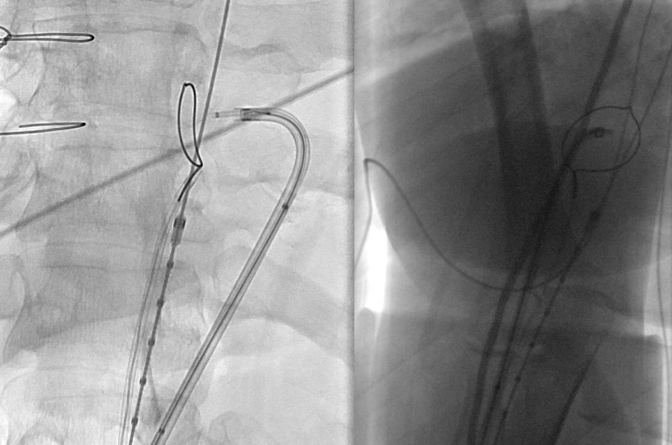
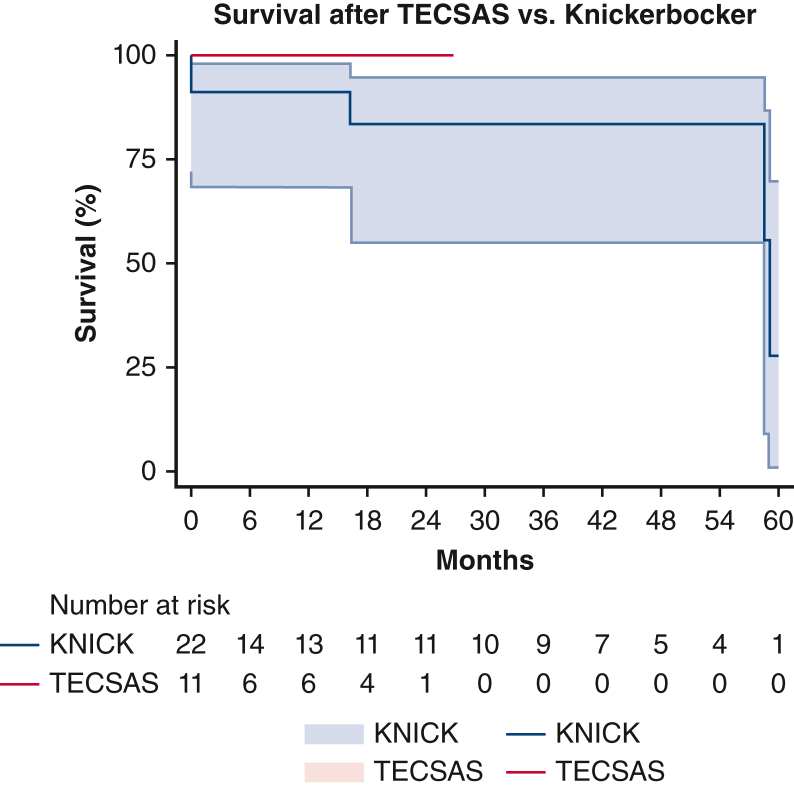
A retrospective review of the Emory Aortic Database from 2016 to 2023 identified 33 patients who underwent TEVAR with intentional endovascular rupture of the dissection flap (Knickerbocker; KNICK) for CTBAD. In 11 patients, we performed transcatheter electrosurgical aortic septostomy (TECSAS) before KNICK. The technical aspects of TECSAS + KNICK are described and results compared with TEVAR + KNICK alone.
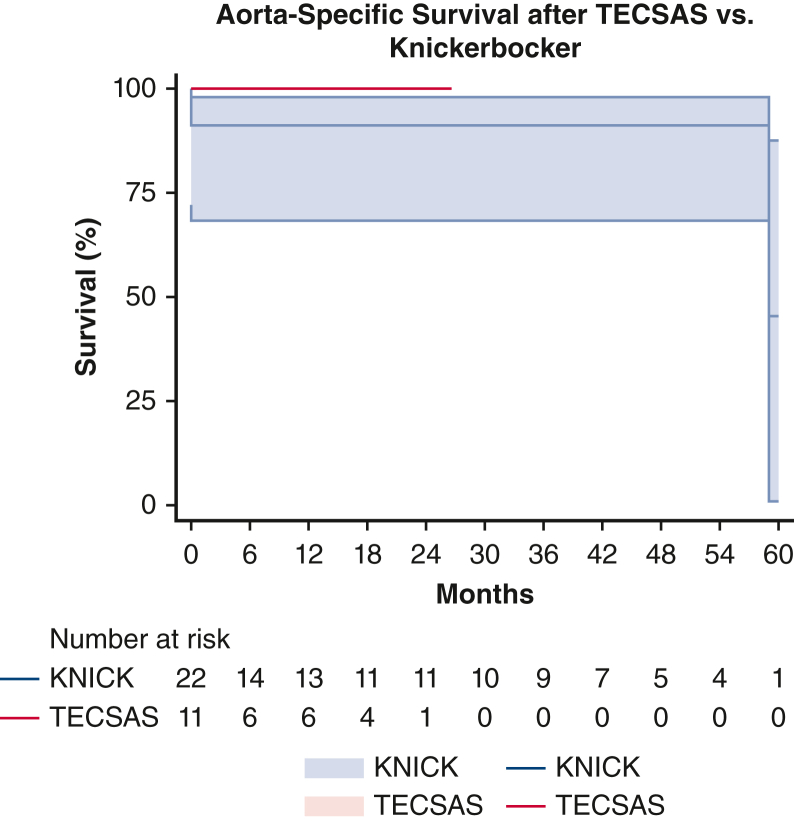
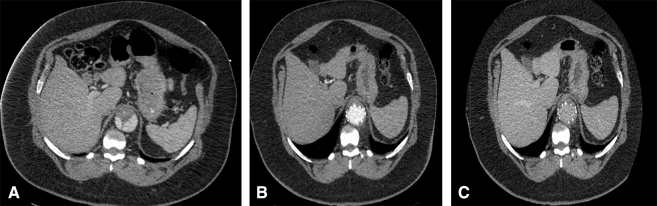
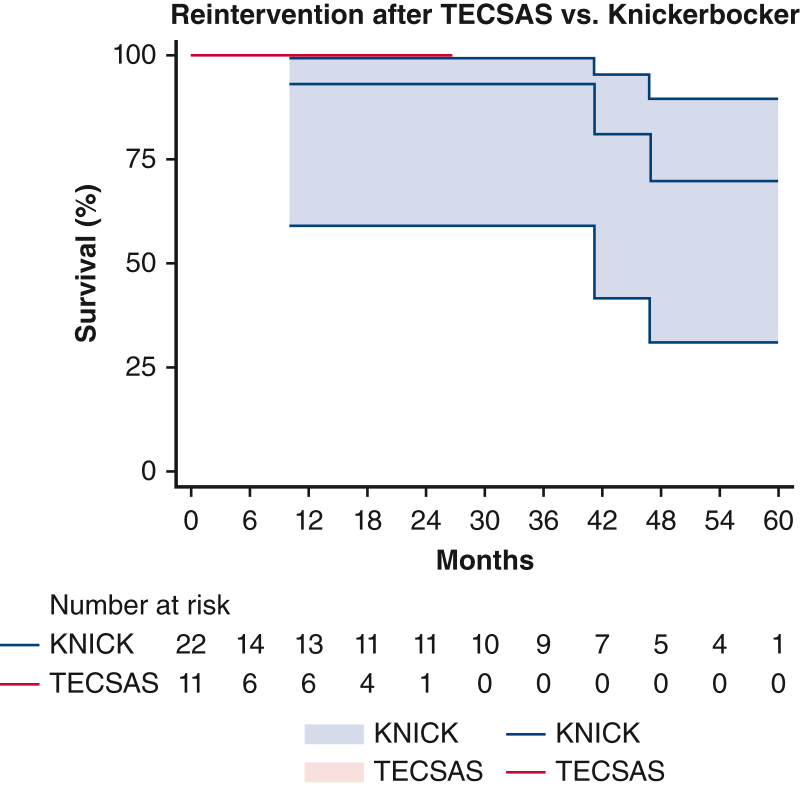
Dissection chronicity, aortic size, and preoperative demographics were similar between groups. Technical success was 100%, with zero stroke or paraplegia in both groups. Thirty-day mortality for TECSAS versus KNICK was 0% versus 13.6% ( = .199). Median follow-up was shorter after TECSAS versus KNICK, although not statistically significant (14.6 months vs 21.9 months; = .065). Elimination of retrograde false lumen perfusion (TECSAS 100% vs KNICK 68.2%; = .035) and complete false lumen thrombosis or obliteration (TECSAS 91.9% vs KNICK 54.6%; = .037) were more frequent after the TECSAS procedure. Aortic reinterventions were less frequent after TECSAS versus KNICK (0% vs 13.6%, = .199), although not statistically significant.
The addition of TECSAS to intentional endovascular rupture of the dissection flap in CTBAD improves distal seal, eliminating retrograde false lumen perfusion. This technique is a safe and precise method to fenestrate a dissection flap and optimize TEVAR in CTBAD.
胸主动脉腔内修复术(TEVAR)治疗慢性B型主动脉夹层(CTBAD)的疗效取决于消除逆行假腔灌注并重塑主动脉。我们描述了一种新型经导管电外科技术在CTBAD中为TEVAR开窗剥离瓣并创建远端密封区的疗效。
对2016年至2023年埃默里主动脉数据库进行回顾性分析,确定33例因CTBAD接受TEVAR并有意进行腔内剥离瓣破裂(尼克博克技术;KNICK)的患者。在11例患者中,我们在KNICK之前进行了经导管电外科主动脉造口术(TECSAS)。描述了TECSAS + KNICK的技术细节,并将结果与单独的TEVAR + KNICK进行比较。
两组间夹层慢性程度、主动脉大小和术前人口统计学特征相似。技术成功率为100%,两组均无卒中或截瘫发生。TECSAS组与KNICK组的30天死亡率分别为0%和13.6%(P = 0.199)。TECSAS组的中位随访时间短于KNICK组,尽管差异无统计学意义(14.6个月对21.9个月;P = 0.065)。TECSAS术后消除逆行假腔灌注(TECSAS组为100%,KNICK组为68.2%;P = 0.035)以及完全假腔血栓形成或闭塞(TECSAS组为91.9%,KNICK组为54.6%;P = 0.037)更为常见。TECSAS术后主动脉再次干预的频率低于KNICK组(0%对13.6%,P = 0.199),尽管差异无统计学意义。
在CTBAD中,在有意进行腔内剥离瓣破裂的基础上增加TECSAS可改善远端密封,消除逆行假腔灌注。该技术是一种安全、精确的开窗剥离瓣并优化CTBAD中TEVAR的方法。