Siqueira Bianca Aparecida, Bredariol Ketlyn Oliveira, Boschiero Matheus Negri, Marson Fernando Augusto Lima
Laboratory of Molecular Biology and Genetics, São Francisco University, Bragança Paulista, Brazil.
Laboratory of Clinical and Molecular Microbiology, São Francisco University, Bragança Paulista, Brazil.
Front Microbiol. 2024 Oct 16;15:1462802. doi: 10.3389/fmicb.2024.1462802. eCollection 2024.
In Brazil, few studies were performed regarding the co-detection of respiratory viruses in hospitalized patients. In this way, the study aimed to describe the epidemiological profile of hospitalized patients due to influenza virus infection that presented co-detection with another respiratory virus.
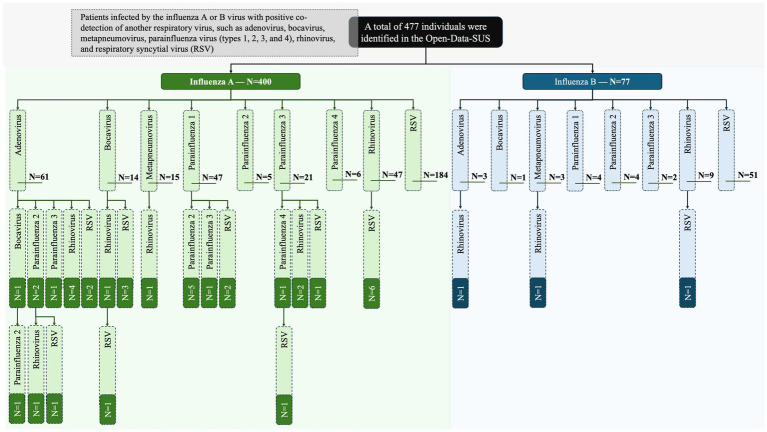
The epidemiological analysis was made by collecting data from Open-Data-SUS. The study comprised patients infected by the influenza A or B virus with positive co-detection of another respiratory virus, such as adenovirus, bocavirus, metapneumovirus, parainfluenza virus (types 1, 2, 3, and 4), rhinovirus, and respiratory syncytial virus (RSV). The markers [gender, age, clinical signs and symptoms, comorbidities, need for intensive care unit (ICU) treatment, and need for ventilatory support] were associated with the chance of death. The data was collected during the first three years of the coronavirus disease (COVID)-19 pandemic-from December 19, 2019, to April 06, 2023.
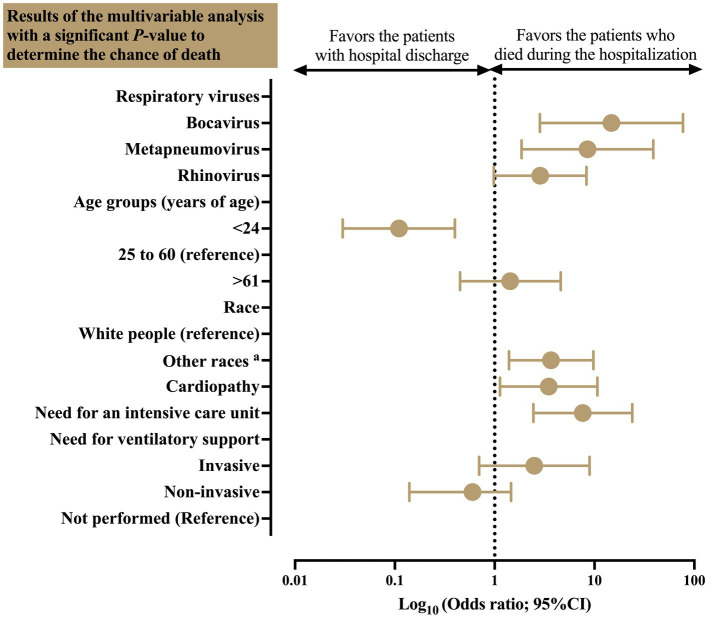
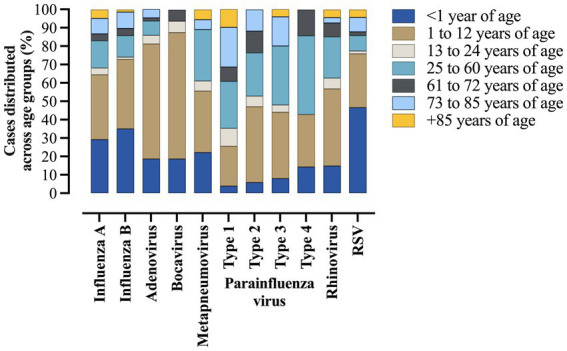
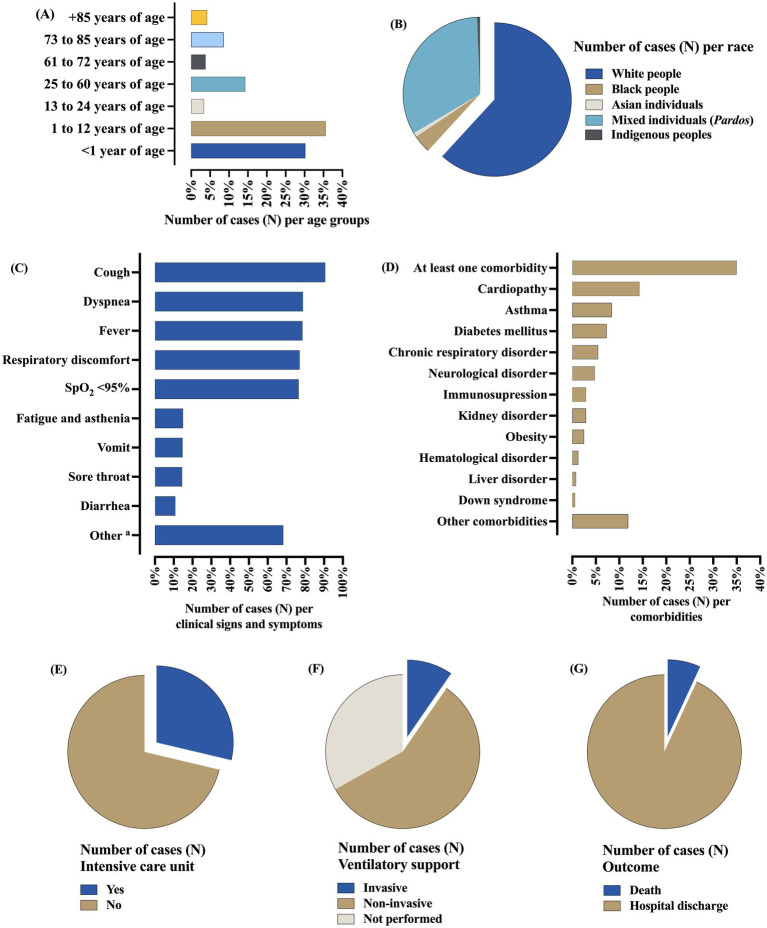
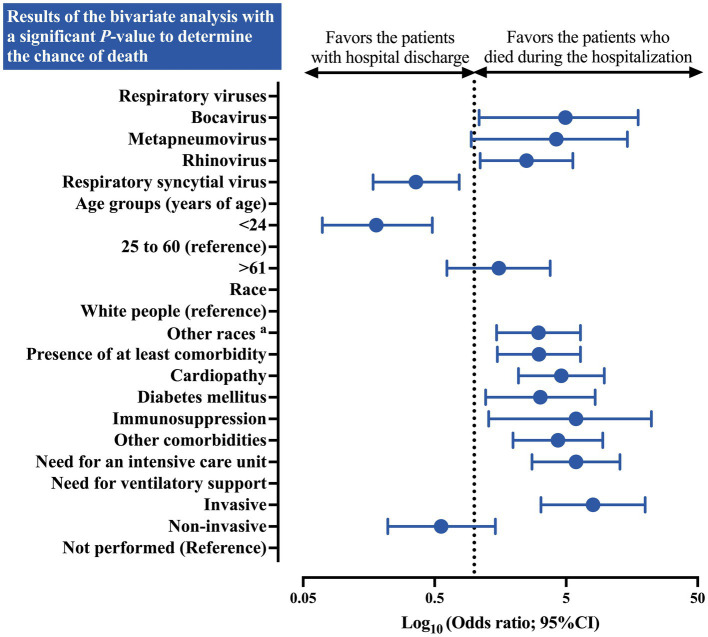
A total of 477 patients were included, among them, the influenza A virus was detected in 400 (83.9%) cases. The co-detection occurred, respectively, for RSV (53.0%), rhinovirus (14.0%), adenovirus (13.4%), parainfluenza virus type 1 (10.7%), parainfluenza virus type 3 (5.2%), metapneumovirus (3.8%), parainfluenza virus type 2 (3.6%), bocavirus (3.4%), and parainfluenza virus type 4 (1.5%). The co-detection rate was higher in the male sex (50.7%), age between 0-12 years of age (65.8%), and white individuals (61.8%). The most common clinical symptoms were cough (90.6%), dyspnea (78.8%), and fever (78.6%). A total of 167 (35.0%) people had at least one comorbidity, mainly cardiopathy (14.3%), asthma (8.4%), and diabetes mellitus (7.3%). The need for ICU treatment occurred in 147 (30.8%) cases, with most of them needing ventilatory support (66.8%), mainly non-invasive ones (57.2%). A total of 33 (6.9%) patients died and the main predictors of death were bocavirus infection (OR = 14.78 [95%CI = 2.84-76.98]), metapneumovirus infection (OR = 8.50 [95%CI = 1.86-38.78]), race (other races vs. white people) (OR = 3.67 [95%CI = 1.39-9.74]), cardiopathy (OR = 3.48 [95%CI = 1.13-10.71]), and need for ICU treatment (OR = 7.64 [95%CI = 2.44-23.92]).
Co-detection between the influenza virus and other respiratory viruses occurred, mainly with RSV, rhinovirus, and adenovirus being more common in men, white people, and in the juvenile phase. Co-detection of influenza virus with bocavirus and metapneumovirus was associated with an increased chance of death. Other factors such as race, cardiopathy, and the need for an ICU were also associated with a higher chance of death.
在巴西,针对住院患者呼吸道病毒合并检测的研究较少。因此,本研究旨在描述因流感病毒感染住院且合并检测出另一种呼吸道病毒的患者的流行病学特征。
通过收集开放数据系统(Open-Data-SUS)的数据进行流行病学分析。该研究纳入了感染甲型或乙型流感病毒且合并检测出另一种呼吸道病毒呈阳性的患者,这些病毒包括腺病毒、博卡病毒、偏肺病毒、副流感病毒(1、2、3和4型)、鼻病毒和呼吸道合胞病毒(RSV)。研究将[性别、年龄、临床症状和体征、合并症、重症监护病房(ICU)治疗需求以及通气支持需求]等指标与死亡几率相关联。数据收集于冠状病毒病(COVID)-19大流行的前三年,即从2019年12月19日至2023年4月6日。
共纳入477例患者,其中400例(83.9%)检测出甲型流感病毒。合并检测分别发生在RSV(53.0%)、鼻病毒(14.0%)、腺病毒(13.4%)、1型副流感病毒(10.7%)、3型副流感病毒(5.2%)、偏肺病毒(3.8%)、2型副流感病毒(3.6%)、博卡病毒(3.4%)和4型副流感病毒(1.5%)。合并检测率在男性(50.7%)、0至12岁年龄组(65.8%)和白人个体(61.8%)中较高。最常见的临床症状为咳嗽(90.6%)、呼吸困难(78.8%)和发热(78.6%)。共有167例(35.0%)患者至少有一种合并症,主要为心脏病(14.3%)、哮喘(8.4%)和糖尿病(7.3%)。147例(30.8%)患者需要ICU治疗,其中大多数需要通气支持(66.8%),主要是无创通气(57.2%)。共有33例(6.9%)患者死亡,死亡的主要预测因素为博卡病毒感染(比值比[OR]=14.78[95%置信区间(CI)=2.84-76.98])、偏肺病毒感染(OR=8.50[95%CI=1.86-38.78])、种族(其他种族与白人相比)(OR=3.67[95%CI=1.39-9.74])、心脏病(OR=3.48[95%CI=1.13-10.71])以及ICU治疗需求(OR=7.64[95%CI=2.44-23.92])。
流感病毒与其他呼吸道病毒之间存在合并检测情况,主要是RSV、鼻病毒和腺病毒,在男性、白人和青少年阶段更为常见。流感病毒与博卡病毒和偏肺病毒的合并检测与死亡几率增加相关。其他因素如种族、心脏病和ICU需求也与较高的死亡几率相关。