Couper Keith, Ji Chen, Deakin Charles D, Fothergill Rachael T, Nolan Jerry P, Long John B, Mason James M, Michelet Felix, Norman Chloe, Nwankwo Henry, Quinn Tom, Slowther Anne-Marie, Smyth Michael A, Starr Kath R, Walker Alison, Wood Sara, Bell Steve, Bradley Gemma, Brown Martina, Brown Shona, Burrow Emma, Charlton Karl, Claxton Dip Andrew, Dra'gon Victoria, Evans Christine, Falloon Jakob, Foster Theresa, Kearney Justin, Lang Nigel, Limmer Matthew, Mellett-Smith Adam, Miller Joshua, Mills Carla, Osborne Ria, Rees Nigel, Spaight Robert E S, Squires Gemma L, Tibbetts Belinda, Waddington Michelle, Whitley Gregory A, Wiles Jason V, Williams Julia, Wiltshire Sarah, Wright Adam, Lall Ranjit, Perkins Gavin D
From the Warwick Medical School, Clinical Trials Unit, University of Warwick (K.C., C.J., J.P.N., J.B.L., J.M.M., F.M., C.N., H.N., A.-M.S., M.A.S., K.R.S., S.W., R.L., G.D.P.), and the Critical Care Unit, University Hospital Coventry and Warwickshire NHS Trust (M.A.S.), Coventry, Devon Air Ambulance (N.L., B.T.) and South Western Ambulance Service NHS Foundation Trust (R.O., S.W.), Exeter, East Midlands Ambulance Service NHS Trust, Nottingham (R.E.S.S., G.L.S., G.A.W.), East of England Ambulance Service NHS Trust, Cambridge (S.B., T.F.), Kingston University (T.Q.) and London Ambulance Service NHS Trust (R.T.F., J.K., J.F., A.M.-S.), London, North East Ambulance Service NHS Foundation Trust, Newcastle upon Tyne (K.C., E.B., M.L.), North West Ambulance Service NHS Trust, Bolton (S.B., A. Wright, M.W.), South Central Ambulance Service NHS Foundation Trust, Bicester (C.D.D., M.B., A.C., V.D.), South East Coast Ambulance Service NHS Foundation Trust, Crawley (G.B., J.W.), Welsh Ambulance Services University NHS Trust, Cwmbran (C.M., N.R.), West Midlands Ambulance Service University NHS Foundation Trust, Brierley Hill (A. Walker, C.E., J.M., J.V.W.), the Critical Care Unit, University Hospitals Birmingham NHS Foundation Trust, Birmingham (G.D.P., K.C.), the Emergency Department, Harrogate and District NHS Foundation Trust, Harrogate (A. Walker), the Department of Anaesthesia, Royal United Hospitals Bath NHS Foundation Trust, Bath (J.P.N.), University Hospital Southampton NHS Foundation Trust, Southampton (C.D.D.), and the University of Bristol, Bristol (J.P.N.) - all in the United Kingdom.
N Engl J Med. 2025 Jan 23;392(4):336-348. doi: 10.1056/NEJMoa2407780. Epub 2024 Oct 31.
In patients with out-of-hospital cardiac arrest, the effectiveness of drugs such as epinephrine is highly time-dependent. An intraosseous route of drug administration may enable more rapid drug administration than an intravenous route; however, its effect on clinical outcomes is uncertain.
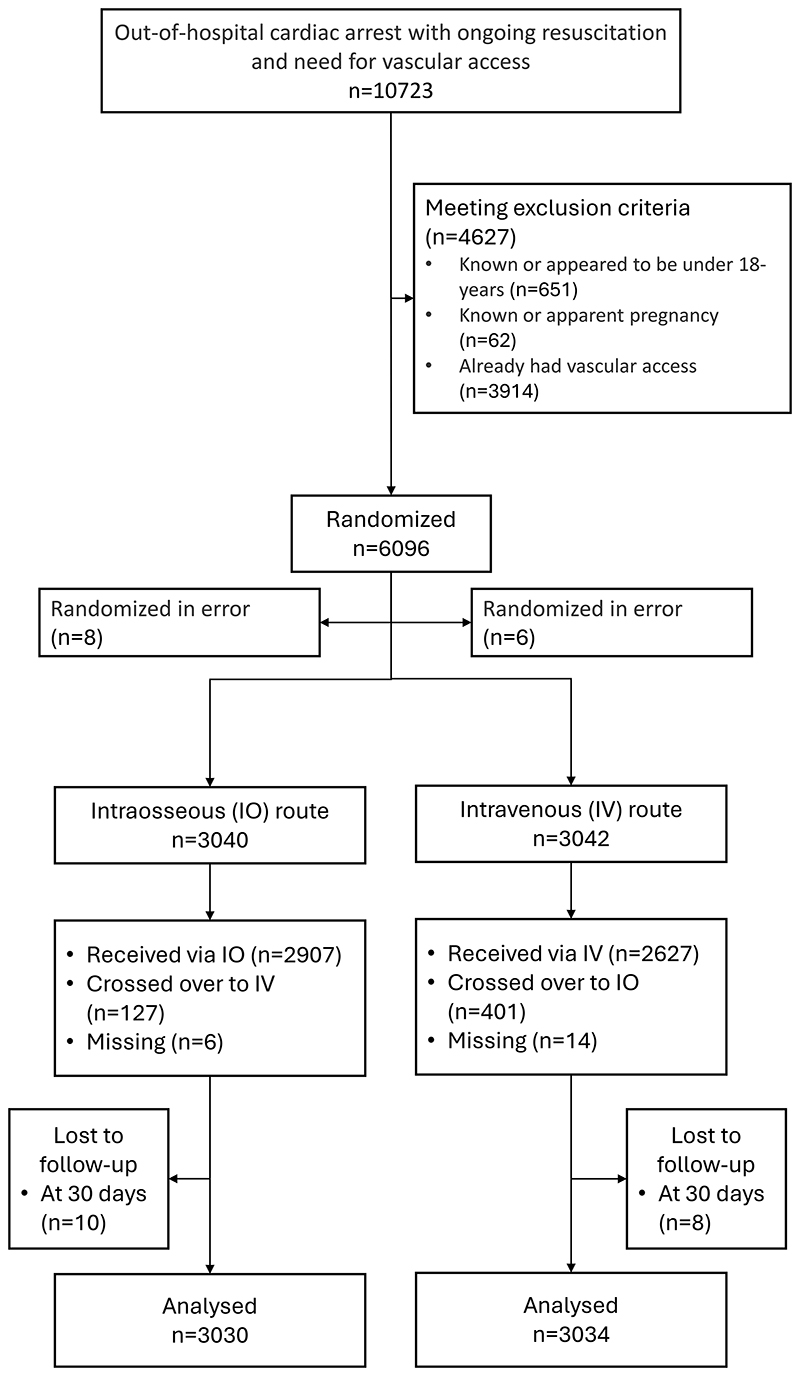
We conducted a multicenter, open-label, randomized trial across 11 emergency medical systems in the United Kingdom that involved adults in cardiac arrest for whom vascular access for drug administration was needed. Patients were randomly assigned to receive treatment from paramedics by means of an intraosseous-first or intravenous-first vascular access strategy. The primary outcome was survival at 30 days. Key secondary outcomes included any return of spontaneous circulation and favorable neurologic function at hospital discharge (defined by a score of 3 or less on the modified Rankin scale, on which scores range from 0 to 6, with higher scores indicating greater disability). No adjustment for multiplicity was made.
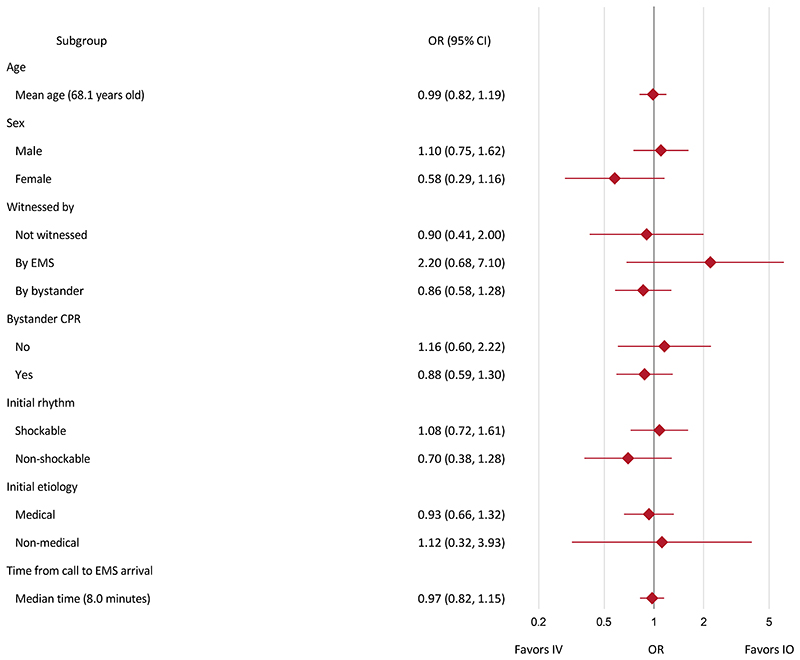
A total of 6082 patients were assigned to a trial group: 3040 to the intraosseous group and 3042 to the intravenous group. At 30 days, 137 of 3030 patients (4.5%) in the intraosseous group and 155 of 3034 (5.1%) in the intravenous group were alive (adjusted odds ratio, 0.94; 95% confidence interval [CI], 0.68 to 1.32; P = 0.74). At the time of hospital discharge, a favorable neurologic outcome was observed in 80 of 2994 patients (2.7%) in the intraosseous group and in 85 of 2986 (2.8%) in the intravenous group (adjusted odds ratio, 0.91; 95% CI, 0.57 to 1.47); a return of spontaneous circulation at any time occurred in 1092 of 3031 patients (36.0%) and in 1186 of 3035 patients (39.1%), respectively (adjusted odds ratio, 0.86; 95% CI, 0.76 to 0.97). During the trial, one adverse event, which occurred in the intraosseous group, was reported.
Among adults with out-of-hospital cardiac arrest requiring drug therapy, the use of an intraosseous-first vascular access strategy did not result in higher 30-day survival than an intravenous-first strategy. (Funded by the National Institute for Health and Care Research; PARAMEDIC-3 ISRCTN Registry number, ISRCTN14223494.).
在院外心脏骤停患者中,肾上腺素等药物的有效性高度依赖时间。骨内给药途径可能比静脉给药途径能更快速地给药;然而,其对临床结局的影响尚不确定。
我们在英国11个紧急医疗系统中进行了一项多中心、开放标签、随机试验,纳入需要血管通路进行药物给药的心脏骤停成年患者。患者被随机分配接受护理人员采用骨内优先或静脉优先血管通路策略的治疗。主要结局是30天生存率。关键次要结局包括任何自主循环恢复以及出院时良好的神经功能(根据改良Rankin量表评分≤3定义,该量表评分范围为0至6,分数越高表明残疾越严重)。未进行多重性调整。
共有6082例患者被分配至试验组:3040例至骨内组,3042例至静脉组。30天时,骨内组3030例患者中有137例(4.5%)存活,静脉组3034例中有155例(5.1%)存活(调整后的优势比为0.94;95%置信区间[CI]为0.68至1.32;P = 0.74)。出院时,骨内组2994例患者中有80例(2.7%)观察到良好的神经学结局,静脉组2986例中有85例(2.8%)(调整后的优势比为0.91;95%CI为0.57至1.47);骨内组3031例患者中有1092例(36.0%)、静脉组3035例患者中有1186例(39.1%)在任何时间出现自主循环恢复(调整后的优势比为0.86;95%CI为0.76至0.97)。试验期间,报告了1例发生在骨内组的不良事件。
在需要药物治疗的院外心脏骤停成年患者中,采用骨内优先血管通路策略并未比静脉优先策略带来更高的30天生存率。(由国家卫生与保健研究所资助;PARAMEDIC - 3国际标准随机对照试验注册编号,ISRCTN14223494。)