Nadkarni Abhijit, Gaikwad Leena, Sequeira Miriam, Javeri Pranay, Benoy Deepthy, Pacheco Marimilha Grace, Velleman Richard, Murthy Pratima, Naughton Felix
Department of Population Health, Centre for Global Mental Health, London School of Hygiene and Tropical Medicine, London, UK.
Addictions and Related Research Group, Sangath, Goa, India.
Nicotine Tob Res. 2025 Mar 24;27(4):575-585. doi: 10.1093/ntr/ntae259.
An estimated 78% of the total deaths attributable to smoking tobacco use occurred in low- and middle-income countries (LMICs) in 2019. In addition, smokeless tobacco increases the risk of all-cause mortality, all cancers, including upper aero-digestive tract cancer, stomach cancer, ischemic heart disease and stroke, with 88% of the mortality burden being borne by the South-East Asian region. Evidence-based interventions from high-income countries (HICs) are not easily transferable to LMICs, as patterns of tobacco use, health beliefs associated with tobacco use, and awareness of specific health risks vary substantially.
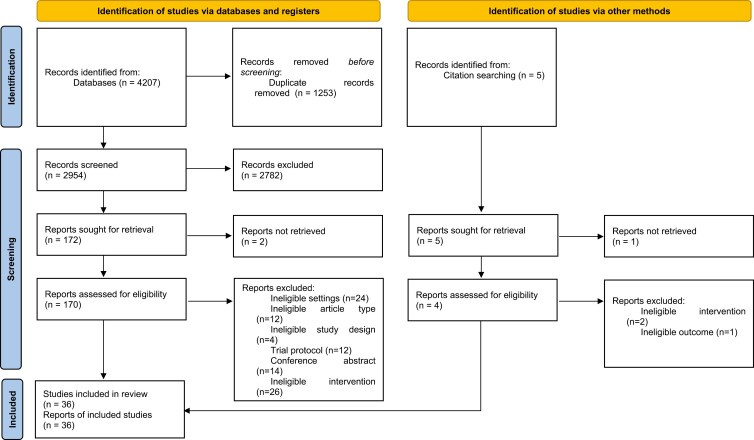
We synthesized the effectiveness of behavioral interventions for tobacco cessation in LMICs through a systematic review and meta-analysis. Interventional studies which delivered individual behavioral intervention and assessed abstinence from tobacco use were included. We examined the pooled intervention effect at 6 months postintervention follow-up.
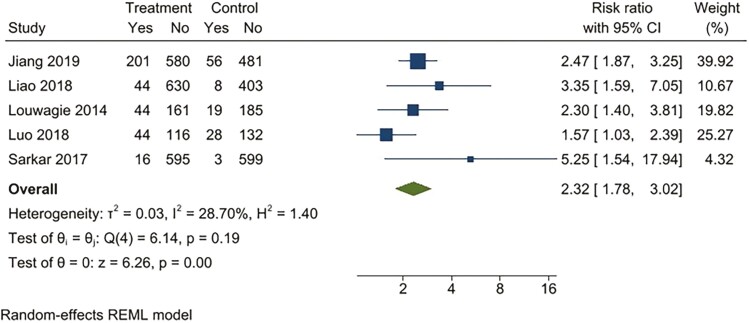
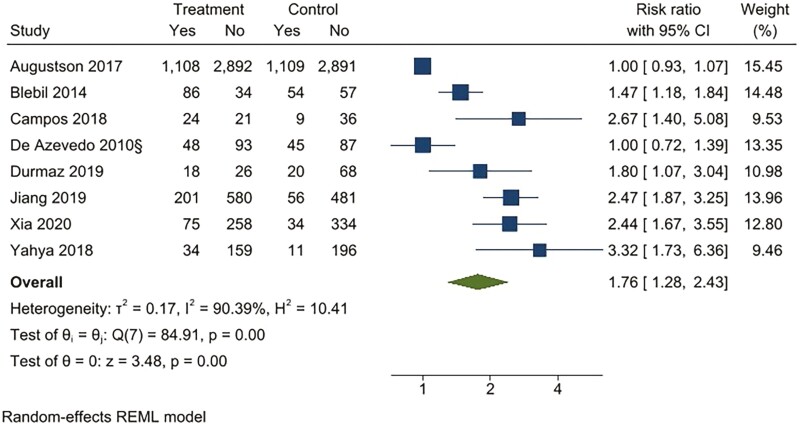
For continuous abstinence at 6 months, the intervention was superior to the active comparator (RR 2.32; 95% CI 1.78 to 3.02) and usual care (RR 4.39; 95% CI 2.38 to 8.11). For point prevalence abstinence at six months, the intervention was superior to the active comparator (RR 1.76; 95% CI 1.28 to 2.44), and usual care (RR 2.37; 95% CI 1.47 to 3.81). The statistical heterogeneity was substantial to considerable for all comparisons. Only six studies had an overall low risk of bias. Publication bias was observed for all comparisons except for 6-month continuous outcomes.
Implementation research is needed to understand factors for programme sustainability and equity of the impact of behavioral interventions in reducing tobacco use in LMICs.
Our review is an important step towards understanding the effectiveness of behavior interventions for tobacco cessation suited for LMICs and which are responsive to the contextual needs of such countries.
2019年,估计因吸烟导致的死亡总数中有78%发生在低收入和中等收入国家(LMICs)。此外,无烟烟草会增加全因死亡率、所有癌症(包括上呼吸道消化道癌症、胃癌、缺血性心脏病和中风)的风险,东南亚地区承担了88%的死亡负担。高收入国家(HICs)基于证据的干预措施不易转移到LMICs,因为烟草使用模式、与烟草使用相关的健康观念以及对特定健康风险的认识差异很大。
我们通过系统评价和荟萃分析,综合了LMICs中戒烟行为干预措施的有效性。纳入了提供个体行为干预并评估戒烟情况的干预性研究。我们在干预后6个月的随访中检查了合并干预效果。
对于6个月时的持续戒烟,干预措施优于积极对照(RR 2.32;95%CI 1.78至3.02)和常规护理(RR 4.39;95%CI 2.38至8.11)。对于6个月时的点患病率戒烟,干预措施优于积极对照(RR 1.76;95%CI 1.28至2.44)和常规护理(RR 2.37;95%CI 1.47至3.81)。所有比较的统计异质性均为中度到高度。只有六项研究的总体偏倚风险较低。除6个月持续结果外,所有比较均观察到发表偏倚。
需要开展实施研究,以了解在LMICs中行为干预在减少烟草使用方面的项目可持续性和影响公平性的因素。
我们的综述是朝着了解适合LMICs且能满足这些国家背景需求的戒烟行为干预措施的有效性迈出的重要一步。